Chronic Eosinophilic Pneumonia Treatments
Find Chronic Eosinophilic Pneumonia Treatments
MethylPREDNISolone
What is Medrol (MethylPREDNISolone)?
Approved To Treat



Related Clinical Trials
Summary: Achilles tendinopathy is a common and often persistent tendon disorder associated with pain, impaired function, and reduced participation in physical activities. Standard care consists of education, load management advice, and progressive calf-strengthening exercises, yet about half of patients remain symptomatic. Corticosteroid injections are frequently used in clinical practice, but evidence on ...
Summary: This phase III trial studies whether inotuzumab ozogamicin added to post-induction chemotherapy and immunotherapy (chemo-immunotherapy) for patients with High-Risk B-cell Acute Lymphoblastic Leukemia (B-ALL) improves outcomes. Inotuzumab ozogamicin is a monoclonal antibody, which is a type of protein that can bind to certain targets on the surface of cells. Inotuzumab ozogamicin is a monoclonal an...
Background: Multiple sclerosis (MS) affects the brain, spinal cord, and optic nerves. MS lesions can appear on the MRI (magnetic resonance imaging) scans in many ways. Sometimes they light up from the outer edge and fill inward. This is called ring enhancement. Researchers think this type of lesion may not heal as well as others. Corticosteroids are the standard treatment to reduce symptoms of MS relapse. But...
Related Latest Advances
Brand Information
- Reduce resistance to new infections
- Exacerbate existing infections
- Increase the risk of disseminated infections
- Increase the risk of reactivation or exacerbation of latent infections
- Mask some signs of infection
- If a MEDROL-treated patient is exposed to varicella, prophylaxis with varicella zoster immune globulin may be indicated. If varicella develops, treatment with antiviral agents may be considered.
- If a MEDROL-treated patient is exposed to measles, prophylaxis with immunoglobulin may be indicated.
- Sodium retention
- Congestive heart failure in susceptible patients
- Hypertension
- Fluid retention
- Potassium loss
- Hypokalemic alkalosis
- Muscle weakness
- Loss of muscle mass
- Steroid myopathy
- Osteoporosis
- Tendon rupture, particularly of the Achilles tendon
- Vertebral compression fractures
- Aseptic necrosis of femoral and humeral heads
- Pathologic fracture of long bones
- Peptic ulcer with possible perforation and hemorrhage
- Pancreatitis
- Abdominal distention
- Ulcerative esophagitis
- Impaired wound healing
- Petechiae and ecchymoses
- May suppress reactions to skin tests
- Thin fragile skin
- Facial erythema
- Increased sweating
- Increased intracranial pressure with papilledema (pseudo-tumor cerebri) usually after treatment
- Convulsions
- Vertigo
- Headache
- Development of Cushingoid state
- Suppression of growth in children
- Secondary adrenocortical and pituitary unresponsiveness, particularly in times of stress, as in trauma, surgery or illness
- Menstrual irregularities
- Decreased carbohydrate tolerance
- Manifestations of latent diabetes mellitus
- Increased requirements of insulin or oral hypoglycemic agents in diabetics
- Posterior subcapsular cataracts
- Increased intraocular pressure
- Glaucoma
- Exophthalmos
- Negative nitrogen balance due to protein catabolism
- Flushing
- Basic principles and indications for corticosteroid therapy should apply. The benefits of ADT should not encourage the indiscriminate use of steroids.
- ADT is a therapeutic technique primarily designed for patients in whom long-term pharmacologic corticoid therapy is anticipated.
- In less severe disease processes in which corticoid therapy is indicated, it may be possible to initiate treatment with ADT. More severe disease states usually will require daily divided high dose therapy for initial control of the disease process. The initial suppressive dose level should be continued until satisfactory clinical response is obtained, usually four to ten days in the case of many allergic and collagen diseases. It is important to keep the period of initial suppressive dose as brief as possible particularly when subsequent use of alternate day therapy is intended.
- Because of the advantages of ADT, it may be desirable to try patients on this form of therapy who have been on daily corticoids for long periods of time (eg, patients with rheumatoid arthritis). Since these patients may already have a suppressed HPA axis, establishing them on ADT may be difficult and not always successful. However, it is recommended that regular attempts be made to change them over. It may be helpful to triple or even quadruple the daily maintenance dose and administer this every other day rather than just doubling the daily dose if difficulty is encountered. Once the patient is again controlled, an attempt should be made to reduce this dose to a minimum.
- As indicated above, certain corticosteroids, because of their prolonged suppressive effect on adrenal activity, are not recommended for alternate day therapy (eg, dexamethasone and betamethasone).
- The maximal activity of the adrenal cortex is between 2 am and 8 am, and it is minimal between 4 pm and midnight. Exogenous corticosteroids suppress adrenocortical activity the least, when given at the time of maximal activity (am).
- In using ADT it is important, as in all therapeutic situations to individualize and tailor the therapy to each patient. Complete control of symptoms will not be possible in all patients. An explanation of the benefits of ADT will help the patient to understand and tolerate the possible flare-up in symptoms which may occur in the latter part of the offsteroid day. Other symptomatic therapy may be added or increased at this time if needed.
- In the event of an acute flare-up of the disease process, it may be necessary to return to a full suppressive daily divided corticoid dose for control. Once control is again established alternate day therapy may be reinstituted.
- Although many of the undesirable features of corticosteroid therapy can be minimized by ADT, as in any therapeutic situation, the physician must carefully weigh the benefit-risk ratio for each patient in whom corticoid therapy is being considered.
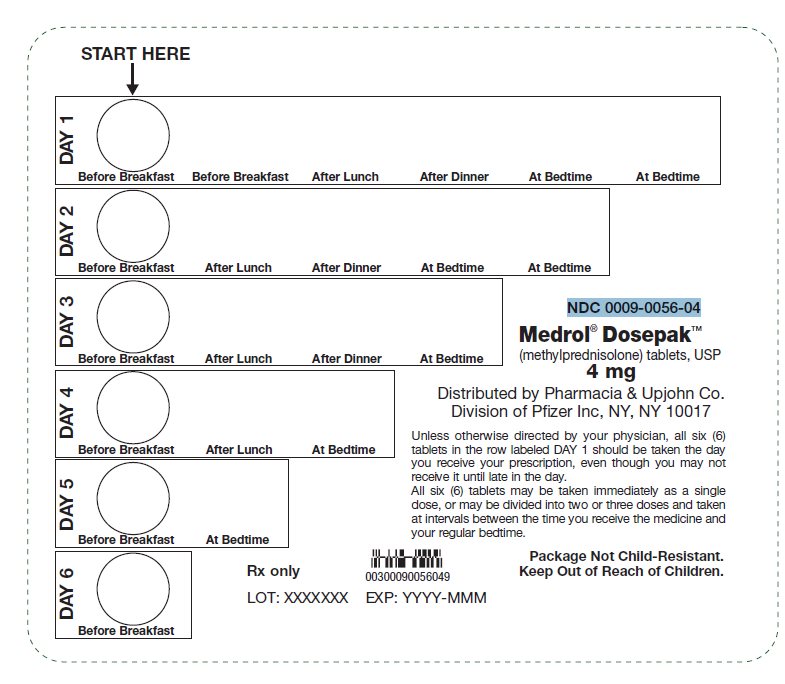
methylprednisolone
tablets, USP
Rx only

methylprednisolone
tablets, USP
Rx only

methylprednisolone
tablets, USP
Rx only

methylprednisolone
tablets, USP
Rx only

methylprednisolone
tablets, USP
Rx only
