Brand Name
Synarel
Generic Name
Nafarelin acetate
View Brand Information FDA approval date: February 13, 1990
Classification: Gonadotropin Releasing Hormone Receptor Agonist
Form: Spray
What is Synarel (Nafarelin acetate)?
FOR CENTRAL PRECOCIOUS PUBERTY SYNAREL is indicated for treatment of central precocious puberty in children of both sexes. The diagnosis of central precocious puberty is suspected when premature development of secondary sexual characteristics occurs at or before the age of 8 years in girls and 9 years in boys, and is accompanied by significant advancement of bone age and/or a poor adult height prediction. The diagnosis should be confirmed by pubertal gonadal sex steroid levels and a pubertal LH response to stimulation by native GnRH. Pelvic ultrasound assessment in girls usually reveals enlarged uterus and ovaries, the latter often with multiple cystic formations. Magnetic resonance imaging or CT-scanning of the brain is recommended to detect hypothalamic or pituitary tumors, or anatomical changes associated with increased intracranial pressure. Other causes of sexual precocity, such as congenital adrenal hyperplasia, testotoxicosis, testicular tumors and/or other autonomous feminizing or masculinizing disorders must be excluded by proper clinical hormonal and diagnostic imaging examinations. FOR ENDOMETRIOSIS SYNAREL is indicated for management of endometriosis, including pain relief and reduction of endometriotic lesions. Experience with SYNAREL for the management of endometriosis has been limited to women 18 years of age and older treated for 6 months.
Approved To Treat
Top Global Experts
There are no experts for this drug
Save this treatment for later
Not sure about your diagnosis?
Tired of the same old research?
Related Clinical Trials
Luteal Phase Support With GnRH Agonist Alone After GnRH Agonist Triggering and Fresh Embryo Transfer Compared to the Reference Protocol (hCG Triggering and Progesterone Luteal Support): a Randomised Controlled Trial
Summary: The development of stimulation protocols for in vitro fertilisation (IVF) has led to a paradox. It has now been established that obtaining a large number of oocytes is a key to success, but that it is also a risk factor for embryo transfer failure after puncture (disruption of endometrial receptivity due to luteal insufficiency) and a risk factor for complications such as ovarian hyperstimulation ...
Related Latest Advances
Brand Information
Synarel (nafarelin acetate)
1DESCRIPTION
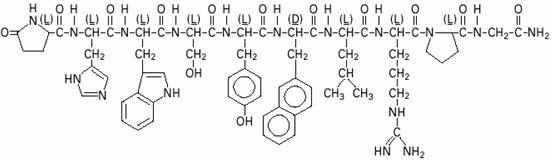
SYNAREL (nafarelin acetate) Nasal Solution is intended for administration as a spray to the nasal mucosa. Nafarelin acetate, the active component of SYNAREL Nasal Solution, is a decapeptide with the chemical name: 5-oxo-
Nafarelin acetate has the following chemical structure:

SYNAREL Nasal Solution contains nafarelin acetate (2 mg/mL, content expressed as nafarelin base) in a solution of benzalkonium chloride, glacial acetic acid, sodium hydroxide or hydrochloric acid (to adjust pH), sorbitol, and purified water.
After priming the pump unit for SYNAREL, each actuation of the unit delivers approximately 100 µL of the spray containing approximately 200 µg nafarelin base. The contents of one spray bottle are intended to deliver at least 60 sprays.
2CLINICAL PHARMACOLOGY
Nafarelin acetate is a potent agonistic analog of gonadotropin-releasing hormone (GnRH). At the onset of administration, nafarelin stimulates the release of the pituitary gonadotropins, LH and FSH, resulting in a temporary increase of gonadal steroidogenesis. Repeated dosing abolishes the stimulatory effect on the pituitary gland. Twice daily administration leads to decreased secretion of gonadal steroids by about 4 weeks; consequently, tissues and functions that depend on gonadal steroids for their maintenance become quiescent.
In
In
After subcutaneous administration of
There appeared to be no significant effect of rhinitis, i.e., nasal congestion, on the systemic bioavailability of SYNAREL; however, if the use of a nasal decongestant for rhinitis is necessary during treatment with SYNAREL, the decongestant should not be used until at least 2 hours following dosing with SYNAREL.
When used regularly in girls and boys with
In clinical studies the peak response of LH to GnRH stimulation was reduced from a pubertal response to a prepubertal response (<15 mlU/mL) within one month of treatment.
Linear growth velocity, which is commonly pubertal in children with CPP, is reduced in most children within the first year of treatment to values of 5 to 6 cm/year or less. Children with CPP are frequently taller than their chronological age peers; height for chronological age approaches normal in most children during the second or third year of treatment with SYNAREL. Skeletal maturation rate (bone age velocity—change in bone age divided by change in chronological age) is usually abnormal (greater than 1) in children with CPP; in most children, bone age velocity approaches normal (1) during the first year of treatment. This results in a narrowing of the gap between bone age and chronological age, usually by the second or third year of treatment. The mean predicted adult height increases.
In clinical trials, breast development was arrested or regressed in 82% of girls, and genital development was arrested or regressed in 100% of boys. Because pubic hair growth is largely controlled by adrenal androgens, which are unaffected by nafarelin, pubic hair development was arrested or regressed only in 54% of girls and boys.
Reversal of the suppressive effects of SYNAREL has been demonstrated to occur in all children with CPP for whom one-year post-treatment follow-up is available (n=69). This demonstration consisted of the appearance or return of menses, the return of pubertal gonadotropin and gonadal sex steroid levels, and/or the advancement of secondary sexual development. Semen analysis was normal in the two ejaculated specimens obtained thus far from boys who have been taken off therapy to resume puberty. Fertility has not been documented by pregnancies and the effect of long-term use of the drug on fertility is not known.
3INDICATIONS AND USAGE FOR CENTRAL PRECOCIOUS PUBERTY
(For Endometriosis,
SYNAREL is indicated for treatment of
The diagnosis of
4CONTRAINDICATIONS
1. Hypersensitivity to GnRH, GnRH agonist analogs or any of the excipients in SYNAREL;
2. Undiagnosed abnormal vaginal bleeding;
3. Use in pregnancy or in women who may become pregnant while receiving the drug. SYNAREL may cause fetal harm when administered to a pregnant woman. Major fetal abnormalities were observed in rats, but not in mice or rabbits after administration of SYNAREL during the period of organogenesis. There was a dose-related increase in fetal mortality and a decrease in fetal weight in rats
4. Use in women who are breast-feeding
5WARNINGS
The diagnosis of central precocious puberty (CPP) must be established before treatment is initiated. Regular monitoring of CPP patients is needed to assess both patient response as well as compliance. This is particularly important during the first 6 to 8 weeks of treatment to assure that suppression of pituitary-gonadal function is rapid. Testing may include LH response to GnRH stimulation and circulating gonadal sex steroid levels. Assessment of growth velocity and bone age velocity should begin within 3 to 6 months of treatment initiation.
Some patients may not show suppression of the pituitary-gonadal axis by clinical and/or biochemical parameters. This may be due to lack of compliance with the recommended treatment regimen and may be rectified by recommending that the dosing be done by caregivers. If compliance problems are excluded, the possibility of gonadotropin independent sexual precocity should be reconsidered and appropriate examinations should be conducted. If compliance problems are excluded and if gonadotropin independent sexual precocity is not present, the dose of SYNAREL may be increased to 1800 µg/day administered as 600 µg tid.
Psychiatric events have been reported in patients taking GnRH agonists. Postmarketing reports with this class of drugs includes symptoms of emotional lability, such as crying, irritability, impatience, anger, and aggression. Monitor for development or worsening of psychiatric symptoms during treatment with SYNAREL.
Post-marketing reports of convulsions have been observed in patients receiving GnRH agonists. These have included patients with a history of seizures, epilepsy, cerebrovascular disorders, central nervous system anomalies or tumors, and patients on concomitant medications that have been associated with convulsions such as bupropion and SSRIs. Convulsions have also been reported in patients in the absence of any of the conditions mentioned above.
Pseudotumor cerebri (idiopathic intracranial hypertension) has been reported in pediatric patients receiving GnRH agonists. Monitor patients for signs and symptoms of pseudotumor cerebri, including headache, papilledema, blurred vision, diplopia, loss of vision, pain behind the eye or pain with eye movement, tinnitus, dizziness, and nausea.
6ADVERSE REACTIONS
In clinical trials of 155 pediatric patients, 2.6% reported symptoms suggestive of drug sensitivity, such as shortness of breath, chest pain, urticaria, rash, and pruritus.
In these 155 patients treated for an average of 41 months and as long as 80 months (6.7 years), adverse events most frequently reported (>3% of patients) consisted largely of episodes occurring during the first 6 weeks of treatment as a result of the transient stimulatory action of nafarelin upon the pituitary-gonadal axis:
- acne (10%)
- transient breast enlargement (8%)
- vaginal bleeding (8%)
- emotional lability (6%)
- transient increase in pubic hair (5%)
- body odor (4%)
- seborrhea (3%)
Hot flashes, common in adult women treated for endometriosis, occurred in only 3% of treated children and were transient. Other adverse events thought to be drug-related, and occurring in >3% of patients were rhinitis (5%) and white or brownish vaginal discharge (3%). Approximately 3% of patients withdrew from clinical trials due to adverse events.
In one male patient with concomitant congenital adrenal hyperplasia, and who had discontinued treatment 8 months previously to resume puberty, adrenal rest tumors were found in the left testis. Relationship to SYNAREL is unlikely.
Regular examinations of the pituitary gland by magnetic resonance imaging (MRI) or computer assisted tomography (CT) of children during long-term nafarelin therapy as well as during the post-treatment period has occasionally revealed changes in the shape and size of the pituitary gland. These changes include asymmetry and enlargement of the pituitary gland, and a pituitary microadenoma has been suspected in a few children. The relationship of these findings to SYNAREL is not known.
7OVERDOSAGE
In experimental animals, a single subcutaneous administration of up to 60 times the recommended human dose (on a µg/kg basis, not adjusted for bioavailability) had no adverse effects. At present, there is no clinical evidence of adverse effects following overdosage of GnRH analogs.
Based on studies in monkeys, SYNAREL is not absorbed after oral administration.
8DOSAGE AND ADMINISTRATION
For the treatment of central precocious puberty (CPP), the recommended daily dose of SYNAREL is 1600 µg. The dose can be increased to 1800 µg daily if adequate suppression cannot be achieved at 1600 µg/day.
The 1600 µg dose is achieved by two sprays (400 µg) into each nostril in the morning (4 sprays) and two sprays into each nostril in the evening (4 sprays), a total of 8 sprays per day. The 1800 µg dose is achieved by 3 sprays (600 µg) into alternating nostrils three times a day, a total of 9 sprays per day. The patient's head should be tilted back slightly, and 30 seconds should elapse between sprays.
If the prescribed therapy has been well tolerated by the patient, treatment of CPP with SYNAREL should continue until resumption of puberty is desired.
There appeared to be no significant effect of rhinitis, i.e., nasal congestion, on the systemic bioavailability of SYNAREL; however, if the use of a nasal decongestant for rhinitis is necessary during treatment with SYNAREL, the decongestant should not be used until at least 2 hours following dosing with SYNAREL.
Sneezing during or immediately after dosing with SYNAREL should be avoided, if possible, since this may impair drug absorption.
At 1600 µg/day, a bottle of SYNAREL provides about a 7-day supply (about 56 sprays). If the daily dose is increased, increase the supply to the patient to ensure uninterrupted treatment for the duration of therapy.
9HOW SUPPLIED
Each 0.5 ounce bottle (NDC 0025-0166-08) contains 8 mL SYNAREL (nafarelin acetate) Nasal Solution 2 mg/mL (as nafarelin base), and is supplied with a metered spray pump that delivers 200 µg of nafarelin per spray. A dust cover and a leaflet of patient instructions are also included.
10DESCRIPTION
SYNAREL (nafarelin acetate) Nasal Solution is intended for administration as a spray to the nasal mucosa. Nafarelin acetate, the active component of SYNAREL Nasal Solution, is a decapeptide with the chemical name: 5-oxo-
Nafarelin acetate has the following chemical structure:
SYNAREL Nasal Solution contains nafarelin acetate (2 mg/mL, content expressed as nafarelin base) in a solution of benzalkonium chloride, glacial acetic acid, sodium hydroxide or hydrochloric acid (to adjust pH), sorbitol, and purified water.
After priming the pump unit for SYNAREL, each actuation of the unit delivers approximately 100 µL of the spray containing approximately 200 µg nafarelin base. The contents of one spray bottle are intended to deliver at least 60 sprays.
11CLINICAL PHARMACOLOGY
Nafarelin acetate is a potent agonistic analog of gonadotropin-releasing hormone (GnRH). At the onset of administration, nafarelin stimulates the release of the pituitary gonadotropins, LH and FSH, resulting in a temporary increase of ovarian steroidogenesis. Repeated dosing abolishes the stimulatory effect on the pituitary gland. Twice daily administration leads to decreased secretion of gonadal steroids by about 4 weeks; consequently, tissues and functions that depend on gonadal steroids for their maintenance become quiescent.
Nafarelin acetate is rapidly absorbed into the systemic circulation after intranasal administration. Maximum serum concentrations (measured by RIA) were achieved between 10 and 40 minutes. Following a single dose of 200 µg base, the observed average peak concentration was 0.6 ng/mL (range 0.2 to 1.4 ng/mL), whereas following a single dose of 400 µg base, the observed average peak concentration was 1.8 ng/mL (range 0.5 to 5.3 ng/mL). Bioavailability from a 400 µg dose averaged 2.8% (range 1.2 to 5.6%). The average serum half-life of nafarelin following intranasal administration is approximately 3 hours. About 80% of nafarelin acetate is bound to plasma proteins at 4°C. Twice daily intranasal administration of 200 or 400 µg of SYNAREL in 18 healthy women for 22 days did not lead to significant accumulation of the drug. Based on the mean C
After subcutaneous administration of
There appeared to be no significant effect of rhinitis, i.e., nasal congestion, on the systemic bioavailability of SYNAREL; however, if the use of a nasal decongestant for rhinitis is necessary during treatment with SYNAREL, the decongestant should not be used until at least 2 hours following dosing of SYNAREL.
In controlled clinical studies, SYNAREL at doses of 400 and 800 µg/day for 6 months was shown to be comparable to danazol, 800 mg/day, in relieving the clinical symptoms of endometriosis (pelvic pain, dysmenorrhea, and dyspareunia) and in reducing the size of endometrial implants as determined by laparoscopy. The clinical significance of a decrease in endometriotic lesions is not known at this time and, in addition, laparoscopic staging of endometriosis does not necessarily correlate with severity of symptoms.
In a single controlled clinical trial, intranasal SYNAREL (nafarelin acetate) at a dose of 400 µg per day was shown to be clinically comparable to intramuscular leuprolide depot, 3.75 mg monthly, for the treatment of the symptoms (dysmenorrhea, dyspareunia and pelvic pain) associated with endometriosis.
SYNAREL 400 µg daily induced amenorrhea in approximately 65%, 80%, and 90% of the patients after 60, 90, and 120 days, respectively. In the first, second, and third post-treatment months, normal menstrual cycles resumed in 4%, 82%, and 100%, respectively, of those patients who did not become pregnant.
At the end of treatment, 60% of patients who received SYNAREL, 400 µg/day, were symptom free, 32% had mild symptoms, 7% had moderate symptoms, and 1% had severe symptoms. Of the 60% of patients who had complete relief of symptoms at the end of treatment, 17% had moderate symptoms 6 months after treatment was discontinued, 33% had mild symptoms, 50% remained symptom free, and no patient had severe symptoms.
During the first two months use of SYNAREL, some women experience vaginal bleeding of variable duration and intensity. In all likelihood, this bleeding represents estrogen withdrawal bleeding and is expected to stop spontaneously. If vaginal bleeding continues, the possibility of lack of compliance with the dosing regimen should be considered. If the patient is complying carefully with the regimen, an increase in dose to 400 µg twice a day should be considered.
There is no evidence that pregnancy rates are enhanced or adversely affected by the use of SYNAREL.
12INDICATIONS AND USAGE FOR ENDOMETRIOSIS
(For Central Precocious Puberty, See
SYNAREL is indicated for management of endometriosis, including pain relief and reduction of endometriotic lesions. Experience with SYNAREL for the management of endometriosis has been limited to women 18 years of age and older treated for 6 months.
13CONTRAINDICATIONS
1. Hypersensitivity to GnRH, GnRH agonist analogs or any of the excipients in SYNAREL;
14WARNINGS
Safe use of nafarelin acetate in pregnancy has not been established clinically. Before starting treatment with SYNAREL, pregnancy must be excluded.
When used regularly at the recommended dose, SYNAREL usually inhibits ovulation and stops menstruation. Contraception is not insured, however, by taking SYNAREL, particularly if patients miss successive doses. Therefore, patients should use nonhormonal methods of contraception. Patients should be advised to see their physician if they believe they may be pregnant. If a patient becomes pregnant during treatment, the drug must be discontinued and the patient must be apprised of the potential risk to the fetus.
Clinical Depression
Depression may occur or worsen during treatment with GnRH agonists including SYNAREL 2 mg/mL. Carefully observe women for depression, especially those with a history of depression and consider whether the risks of continuing SYNAREL 2 mg/mL outweigh the benefits. Women with new or worsening depression should be referred to a mental health professional, as appropriate
15OVERDOSAGE
In experimental animals, a single subcutaneous administration of up to 60 times the recommended human dose (on a µg/kg basis, not adjusted for bioavailability) had no adverse effects. At present, there is no clinical evidence of adverse effects following overdosage of GnRH analogs.
Based on studies in monkeys, SYNAREL is not absorbed after oral administration.
16DOSAGE AND ADMINISTRATION
For the management of endometriosis, the recommended daily dose of SYNAREL is 400 µg. This is achieved by one spray (200 µg) into one nostril in the morning and one spray into the other nostril in the evening. Treatment should be started between days 2 and 4 of the menstrual cycle.
In an occasional patient, the 400 µg daily dose may not produce amenorrhea. For these patients with persistent regular menstruation after 2 months of treatment, the dose of SYNAREL may be increased to 800 µg daily. The 800 µg dose is administered as one spray into each nostril in the morning (a total of two sprays) and again in the evening.
The recommended duration of administration is six months. Retreatment cannot be recommended since safety data for retreatment are not available. If the symptoms of endometriosis recur after a course of therapy, and further treatment with SYNAREL is contemplated, it is recommended that bone density be assessed before retreatment begins to ensure that values are within normal limits.
There appeared to be no significant effect of rhinitis, i.e., nasal congestion, on the systemic bioavailability of SYNAREL; however, if the use of a nasal decongestant for rhinitis is necessary during treatment with SYNAREL, the decongestant should not be used until at least 2 hours following dosing with SYNAREL.
Sneezing during or immediately after dosing with SYNAREL should be avoided, if possible, since this may impair drug absorption.
At 400 µg/day, a bottle of SYNAREL provides a 30-day (about 60 sprays) supply. If the daily dose is increased, increase the supply to the patient to ensure uninterrupted treatment for the recommended duration of therapy.
17HOW SUPPLIED
Each 0.5 ounce bottle (NDC 0025-0166-08) contains 8 mL SYNAREL (nafarelin acetate) Nasal Solution 2 mg/mL (as nafarelin base), and is supplied with a metered spray pump that delivers 200 µg of nafarelin per spray. A dust cover and a leaflet of patient instructions are also included.
18PRINCIPAL DISPLAY PANEL - 8 mL Bottle Label
ALWAYS DISPENSE WITH MEDICATION GUIDE
Pfizer
Synarel
2 mg/mL (as nafarelin base)
SPRAY - FOR INTRANASAL USE ONLY.
8 mL (60 metered sprays)
19PRINCIPAL DISPLAY PANEL - 8 mL Bottle Carton
ALWAYS DISPENSE WITH MEDICATION GUIDE
Pfizer
Synarel
2 mg/mL (as nafarelin base)
SPRAY – FOR INTRANASAL USE ONLY
Each actuation delivers approximately
Carton contains: 1 bottle of nasal solution with
Store upright.
8 mL (60 metered sprays)