Brand Name
Relafen
Generic Name
Nabumetone
View Brand Information FDA approval date: February 25, 2002
Classification: Nonsteroidal Anti-inflammatory Drug
Form: Tablet
What is Relafen (Nabumetone)?
Carefully consider the potential benefits and risks of nabumetone tablets and other treatment options before deciding to use nabumetone tablets. Use the lowest effective dose for the shortest duration consistent with individual patient treatment goals. Nabumetone tablets, USP are indicated: For relief of the signs and symptoms of rheumatoid arthritis. For relief of the signs and symptoms of osteoarthritis.
Approved To Treat
Top Global Experts
There are no experts for this drug
Save this treatment for later
Not sure about your diagnosis?
Related Clinical Trials
There is no clinical trials being done for this treatment
Related Latest Advances
There is no latest advances for this treatment
Brand Information
RELAFEN DS (NABUMETONE)
1DESCRIPTION
Nabumetone is a naphthylalkanone designated chemically as 4-(6-methoxy-2-naphthalenyl)-2-butanone. It has the following structure:
Nabumetone is a white to off-white crystalline substance. It is nonacidic and practically insoluble in water, but soluble in alcohol and most organic solvents. It has an n-octanol:phosphate buffer partition coefficient of 2,400 at pH 7.4.
Each tablet, for oral administration, contains either 500 mg, 750 mg, or 1000 mg of nabumetone. In addition, each tablet contains the following inactive ingredients: povidone, croscarmellose, magnesium stearate, sodium lauryl sulfate, and colloidal silicon dioxide. The coating contains hydroxypropyl cellulose and hypromellose.
2CLINICAL PHARMACOLOGY
Nabumetone is a non-steroidal anti-inflammatory drug (NSAID) that exhibits anti-inflammatory, analgesic, and antipyretic properties in pharmacologic studies. As with other non-steroidal anti-inflammatory agents, its mode of action is not known; however, the ability to inhibit prostaglandin synthesis may be involved in the anti-inflammatory effect.
The parent compound is a prodrug, which undergoes hepatic biotransformation to the active component, 6-methoxy-2-naphthylacetic acid (6MNA), that is a potent inhibitor of prostaglandin synthesis.
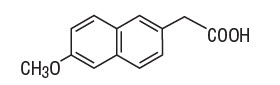
6-methoxy-2-naphthylacetic acid (6MNA)
It is acidic and has an n-octanol:phosphate buffer partition coefficient of 0.5 at pH 7.4.
2.1Pharmacokinetics
After oral administration, approximately 80% of a radiolabeled dose of nabumetone is found in the urine, indicating that nabumetone is well absorbed from the gastrointestinal tract. Nabumetone itself is not detected in the plasma because, after absorption, it undergoes rapid biotransformation to the principal active metabolite, 6-methoxy-2-naphthylacetic acid (6MNA). Approximately 35% of a 1,000 mg oral dose of nabumetone is converted to 6MNA and 50% is converted into unidentified metabolites which are subsequently excreted in the urine. Following oral administration of nabumetone, 6MNA exhibits pharmacokinetic characteristics that generally follow a one-compartment model with first order input and first order elimination.
6MNA is more than 99% bound to plasma proteins. The free fraction is dependent on total concentration of 6MNA and is proportional to dose over the range of 1,000 mg to 2,000 mg. It is 0.2% to 0.3% at concentrations typically achieved following administration of 1,000 mg of nabumetone and is approximately 0.6% to 0.8% of the total concentrations at steady state following daily administration of 2,000 mg.
Steady-state plasma concentrations of 6MNA are slightly lower than predicted from single-dose data. This may result from the higher fraction of unbound 6MNA which undergoes greater hepatic clearance.
Coadministration of food increases the rate of absorption and subsequent appearance of 6MNA in the plasma but does not affect the extent of conversion of nabumetone into 6MNA. Peak plasma concentrations of 6MNA are increased by approximately one third.
Coadministration with an aluminum-containing antacid had no significant effect on the bioavailability of 6MNA.
The simulated curves in the graph below illustrate the range of active metabolite plasma concentrations that would be expected from 95% of patients following 1,000 mg to 2,000 mg doses to steady state. The cross-hatched area represents the expected overlap in plasma concentrations due to intersubject variation following oral administration of 1,000 mg to 2,000 mg of nabumetone.
6MNA undergoes biotransformation in the liver, producing inactive metabolites that are eliminated as both free metabolites and conjugates. None of the known metabolites of 6MNA has been detected in plasma. Preliminary
Following oral administration of dosages of 1,000 mg to 2,000 mg to steady state, the mean plasma clearance of 6MNA is 20 to 30 mL/min and the elimination half-life is approximately 24 hours.
2.1.1Elderly Patients
Steady-state plasma concentrations in elderly patients were generally higher than in young healthy subjects (see
2.1.2Renal Insufficiency
In moderate renal insufficiency patients (creatinine clearance 30 to 49 mL/min), the terminal half-life of 6MNA was increased by approximately 50% (39.2 ± 7.8 hrs, N = 12) compared to the normal subjects (26.9 ± 3.3 hrs, N = 13), and there was a 50% increase in the plasma levels of unbound 6MNA.
Additionally, the renal excretion of 6MNA in the moderate renal impaired patients decreased on average by 33% compared to that in the normal patients. A similar increase in the mean terminal half-life of 6MNA was seen in a small study of patients with severe renal dysfunction (creatinine clearance < 30 mL/min). In patients undergoing hemodialysis, steady-state plasma concentrations of the active metabolite 6MNA were similar to those observed in healthy subjects. Due to extensive protein binding, 6MNA is not dialyzable.
Dosage adjustment of nabumetone generally is not necessary in patients with mild renal insufficiency (≥ 50 mL/min). Caution should be used in prescribing nabumetone to patients with moderate or severe renal insufficiency. The maximum starting doses of nabumetone in patients with moderate or severe renal insufficiency should not exceed 750 mg or 500 mg, respectively once daily. Following careful monitoring of renal function in patients with moderate or severe renal insufficiency, daily doses may be increased to a maximum of 1,500 mg and 1,000 mg, respectively [see
2.1.3Hepatic Impairment
Data in patients with severe hepatic impairment are limited. Biotransformation of nabumetone to 6MNA and the further metabolism of 6MNA to inactive metabolites is dependent on hepatic function and could be reduced in patients with severe hepatic impairment (history of or biopsy-proven cirrhosis).
3INDICATIONS AND USAGE
Carefully consider the potential benefits and risks of nabumetone tablets and other treatment options before deciding to use nabumetone tablets. Use the lowest effective dose for the shortest duration consistent with individual patient treatment goals [see
Nabumetone tablets are indicated for relief of signs and symptoms of osteoarthritis and rheumatoid arthritis
4CONTRAINDICATIONS
Nabumetone tablets are contraindicated in patients with known hypersensitivity to nabumetone or product excipients.
Nabumetone tablets should not be given to patients who have experienced asthma, urticaria, or allergic-type reactions after taking aspirin or other NSAIDs. Severe, rarely fatal, anaphylactic-like reactions to NSAIDs have been reported in such patients [see
Nabumetone tablets are contraindicated in the setting of coronary artery bypass graft (CABG) surgery [see
5ADVERSE REACTIONS
To report SUSPECTED ADVERSE REACTIONS, contact Carwin Pharmaceutical Associates at 1-844-700-5011 or www.carwinpharma.com or FDA at 1-800-FDA-1088 or www.fda.gov/medwatch.
Adverse reaction information was derived from blinded-controlled and open-labeled clinical trials and from worldwide marketing experience. In the description below, rates of the more common events (greater than 1%) and many of the less common events (less than 1%) represent results of U.S. clinical studies.
Of the 1,677 patients who received nabumetone during U.S. clinical trials, 1,524 were treated for at least 1 month, 1,327 for at least 3 months, 929 for at least a year, and 750 for at least 2 years. More than 300 patients have been treated for 5 years or longer.
The most frequently reported adverse reactions were related to the gastrointestinal tract and included diarrhea, dyspepsia, and abdominal pain.
6OVERDOSAGE
Symptoms following acute NSAIDs overdoses are usually limited to lethargy, drowsiness, nausea, vomiting, and epigastric pain, which are generally reversible with supportive care. Gastrointestinal bleeding can occur. Hypertension, acute renal failure, respiratory depression, and coma may occur, but are rare. Anaphylactoid reactions have been reported with therapeutic ingestion of NSAIDs and may occur following an overdose.
Patients should be managed by symptomatic and supportive care following a NSAIDs overdose. There are no specific antidotes. Emesis and/or activated charcoal (60 to 100 grams in adults, 1 to 2 g/kg in children), and/or osmotic cathartic may be indicated in patients seen within 4 hours of ingestion with symptoms or following a large overdose (5 to 10 times the usual dose). Forced diuresis, alkalinization of urine, hemodialysis, or hemoperfusion may not be useful due to high protein binding.
There have been overdoses of up to 25 grams of Nabumetone reported with no long-term sequelae following standard emergency treatment (i.e., activated charcoal, gastric lavage, IV H
7DOSAGE AND ADMINISTRATION
Carefully consider the potential benefits and risks of nabumetone tablets and other treatment options before deciding to use nabumetone tablets. Use the lowest effective dose for the shortest duration consistent with individual patient treatment goals [see
After observing the response to initial therapy with nabumetone tablets, the dose and frequency should be adjusted to suit an individual patient's needs.
7.1Osteoarthritis and Rheumatoid Arthritis
The recommended starting dose is 1,000 mg taken as a single dose with or without food. Some patients may obtain more symptomatic relief from 1,500 mg to 2,000 mg per day. Nabumetone tablets can be given in either a single or twice-daily dose. Dosages greater than 2,000 mg per day have not been studied. The lowest effective dose should be used for chronic treatment [see
8HOW SUPPLIED
Nabumetone Tablets USP, 1000 mg are white, coated, modified capsule-shaped tablets, deep bisect on one side and debossed logo "NB 1000" on the other. They are available in bottles of:
100 tablets – NDC 15370-170-10
60 tablets – NDC 15370-170-60
30 tablets – NDC 15370-170-30
9PRINCIPAL DISPLAY PANEL - 1,000 mg Tablet Bottle Label
NDC 15370-170-30
RELAFEN
PHARMACIST: PLEASE DISPENSE WITH
30 Tablets
carwin