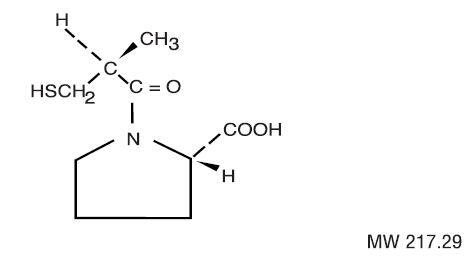
Captopril
View Brand InformationWhat is Captopril?
Approved To Treat
Top Global Experts




Related Clinical Trials
Summary: Primary aldosteronism is a prevalent yet underdiagnosed cause of secondary hypertension, contributing to significant cardiovascular morbidity and renal dysfunction. Despite affecting up to 20% of hypertensive patients, PA is frequently missed because it lacks distinctive clinical features and often presents with nonspecific symptoms like resistant hypertension or subtle electrolyte imbalances. The...
Summary: The aim of this protocol is to assess the presence and severity of primary aldosteronism pathophysiology in patients with type 2 diabetes who have, or are at-risk for developing, chronic kidney disease.
Summary: 1. to investigate the association between route of administration of exogenous estrogen (transdermal vs. oral) and cardiorenal risk in cisgender (gender identity aligning with sex at birth) and transgender (gender identity not aligning with sex at birth) women. 2. to investigate the association between exogenous testosterone exposure and cardiorenal risk in cisgender (gender identity aligning with...
Related Latest Advances
Brand Information
- When pregnancy is detected, discontinue captopril tablets as soon as possible.
- Drugs that act directly on the renin-angiotensin system can cause injury and death to the developing fetus. See

Tablets, USP
Captopril, USP.................................................................. 12.5 mg
15° to 30°C (59° to 86°F) [see USP Controlled Room Temperature].
Protect from light and moisture.


Tablets, USP
Captopril, USP..................................................................... 25 mg
15° to 30°C (59° to 86°F) [see USP Controlled Room Temperature].
Protect from light and moisture.
