Brand Name
Lovastatin
View Brand InformationFDA approval date: December 17, 2001
Classification: HMG-CoA Reductase Inhibitor
Form: Tablet
What is Lovastatin?
Therapy with lovastatin should be a component of multiple risk factor intervention in those individuals with dyslipidemia at risk for atherosclerotic vascular disease. Lovastatin should be used in addition to a diet restricted in saturated fat and cholesterol as part of a treatment strategy to lower total-C and LDL-C to target levels when the response to diet and other nonpharmacological measures alone has been inadequate to reduce risk. Primary Prevention of Coronary Heart Disease In individuals without symptomatic cardiovascular disease, average to moderately elevated total-C and LDL-C, and below average HDL-C, lovastatin is indicated to reduce the risk of: Myocardial infarction Unstable angina Coronary revascularization procedures Coronary Heart Disease Lovastatin is indicated to slow the progression of coronary atherosclerosis in patients with coronary heart disease as part of a treatment strategy to lower total-C and LDL-C to target levels. Hypercholesterolemia Therapy with lipid-altering agents should be a component of multiple risk factor intervention in those individuals at significantly increased risk for artherosclerotic vascular disease due to hypercholesterolemia. Lovastatin is indicated as an adjunct to diet for the reduction of elevated total-C and LDL-C levels in patients with primary hypercholesterolemia , when the response to diet restricted in saturated fat and cholesterol and to other nonpharmacological measures alone has been inadequate. 2 Classification of Hyperlipoproteinemias Lipid Elevaions Type Lipoproteins elevated major minor I chylonicrons TG ↑→C IIa LDL C -- IIb LDL, VLDL C TG III IDL C/TG -- IV VLDL TG ↑→C V chylomicrons, VLDL TG ↑→C IDL = intermediate-densit lipoprotein Adolescent Patients with Heterozygous Familial Hypercholesterolemia Lovastatin is indicated as an adjunct to diet to reduce total-C, LDL-C and apolipoprotein B levels in adolescent boys and girls who are at least one year post-menarche, 10 to 17 years of age, with heFH if after an adequate trial of diet therapy the following findings are present: LDL-C remains >189 mg/dL or LDL-C remains >160 mg/dL and: there is a positive family history of premature cardiovascular disease or two or more other CVD risk factors are present in the adolescent patient General Recommendations Prior to initiating therapy with lovastatin, secondary causes for hypercholesterolemia should be excluded, and a lipid profile performed to measure total-C, HDL-C, and TG. For patients with TG less than 400 mg/dL.
Approved To Treat
Top Global Experts
There are no experts for this drug
Save this treatment for later
Not sure about your diagnosis?
Related Clinical Trials
There is no clinical trials being done for this treatment
Related Latest Advances
There is no latest advances for this treatment
Brand Information
Lovastatin (Lovastatin)
1DESCRIPTION
Lovastatin is a cholesterol lowering agent isolated from a strain of
Lovastatin is [1
Lovastatin is a white, nonhygroscopic crystalline powder that is insoluble in water and sparingly soluble in ethanol, methanol, and acetonitrile.
Lovastatin tablets are supplied as 10 mg, 20 mg and 40 mg tablets for oral administration. In addition, each tablet contains the following inactive ingredients: lactose monohydrate, magnesium stearate, microcrystalline cellulose, poloxamer, pregelatinized cornstarch, sodium starch glycolate, butylated hydroxyaniso and talc. Butylated hydroxyanisole (BHA) is added as a preservative.
2CLINICAL PHARMACOLOGY
The involvement of low-density lipoprotein cholesterol (LDL-C) in atherogenesis has been well-documented in clinical and pathological studies, as well as in many animal experiments. Epidemiological and clinical studies have established that high LDL-C and low high-density lipoprotein cholesterol (HDL-C) are both associated with coronary heart disease. However, the risk of developing coronary heart disease is continuous and graded over the range of cholesterol levels and many coronary events do occur in patients with total cholesterol (total-C) and LDL-C in the lower end of this range.
Lovastatin has been shown to reduce both normal and elevated LDL-C concentrations. LDL is formed from very low-density lipoprotein (VLDL) and is catabolized predominantly by the high affinity LDL receptor. The mechanism of the LDL-lowering effect of lovastatin may involve both reduction of VLDL-C concentration, and induction of the LDL receptor, leading to reduced production and/or increased catabolism of LDL-C. Apolipoprotein B also falls substantially during treatment with lovastatin. Since each LDL particle contains one molecule of apolipoprotein B, and since little apolipoprotein B is found in other lipoproteins, this strongly suggests that lovastatin does not merely cause cholesterol to be lost from LDL, but also reduces the concentration of circulating LDL particles. In addition, lovastatin can produce increases of variable magnitude in HDL-C, and modestly reduces VLDL-C and plasma triglycerides (TG) (see
Lovastatin is a specific inhibitor of HMG-CoA reductase, the enzyme which catalyzes the conversion of HMG-CoA to mevalonate. The conversion of HMG-CoA to mevalonate is an early step in the biosynthetic pathway for cholesterol.
2.1Pharmacokinetics
Lovastatin is a lactone, which is readily hydrolyzed
Following an oral dose of
Both lovastatin and its β-hydroxyacid metabolite are highly bound (>95%) to human plasma proteins. Animal studies demonstrated that lovastatin crosses the blood-brain and placental barriers.
The major active metabolites present in human plasma are the β-hydroxyacid of lovastatin, its 6'-hydroxy derivative, and two additional metabolites. Peak plasma concentrations of both active and total inhibitors were attained within 2 to 4 hours of dose administration. While the recommended therapeutic dose range is 10 to 80 mg/day, linearity of inhibitory activity in the general circulation was established by a single dose study employing lovastatin tablet dosages from 60 to as high as 120 mg. With a once-a-day dosing regimen, plasma concentrations of total inhibitors over a dosing interval achieved a steady state between the second and third days of therapy and were about 1.5 times those following a single dose. When lovastatin was given under fasting conditions, plasma concentrations of total inhibitors were on average about two-thirds those found when lovastatin was administered immediately after a standard test meal.
In a study of patients with severe renal insufficiency (creatinine clearance 10 to 30 mL/min), the plasma concentrations of total inhibitors after a single dose of lovastatin were approximately two-fold higher than those in healthy volunteers.
In a study including 16 elderly patients between 70 to 78 years of age who received lovastatin 80 mg/day, the mean plasma level of HMG-CoA reductase inhibitory activity was increased approximately 45% compared with 18 patients between 18 to 30 years of age (see
Although the mechanism is not fully understood, cyclosporine has been shown to increase the AUC of HMG-CoA reductase inhibitors. The increase in AUC for lovastatin and lovastatin acid is presumably due, in part, to inhibition of CYP3A4.
The risk of myopathy is increased by high levels of HMG-CoA reductase inhibitory activity in plasma. Strong inhibitors of CYP3A4 can raise the plasma levels of HMG-CoA reductase inhibitory activity and increase the risk of myopathy (see
Lovastatin is a substrate for cytochrome P450 isoform 3A4 (CYP3A4) (see
** Kantola, T, et al., Clin Pharmacol Ther 1998; 63(4):397-402.
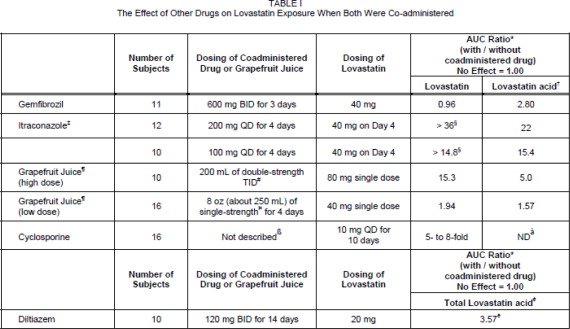
* Results based on a chemical assay.
† Lovastatin acid refers to the β-hydroxyacid of lovastatin.
‡ The mean total AUC of lovastatin without itraconazole phase could not be determined accurately. Results could be representative of strong CYP3A4 inhibitors such as ketoconazole, posaconazole, clarithromycin, telithromycin, HIV protease inhibitors, and nefazodone.
§ Estimated minimum change.
¶ The effect of amounts of grapefruit juice between those used in these two studies on lovastatin pharmacokinetics has not been studied.
# Double-strength: one can of frozen concentrate diluted with one can of water.
Grapefruit juice was administered TID for 2 days, and 200 mL together with single dose lovastatin and 30 and 90 minutes following single dose lovastatin on Day 3.
Þ Single-strength: one can of frozen concentrate diluted with 3 cans of water. Grapefruit juice was administered with breakfast for 3 days, and lovastatin was administered in the evening on Day 3.
ß Cyclosporine-treated patients with psoriasis or post kidney or heart transplant patients with stable graft function, transplanted at least 9 months prior to study.
à ND = Analyte not determined.
è Lactone converted to acid by hydrolysis prior to analysis. Figure represents total unmetabolized acid and lactone.
2.1.1Clinical Studies in Adults
Lovastatin has been shown to be highly effective in reducing total-C and LDL-C in heterozygous familial and non-familial forms of primary hypercholesterolemia and in mixed hyperlipidemia. A marked response was seen within 2 weeks, and the maximum therapeutic response occurred within 4 to 6 weeks. The response was maintained during continuation of therapy. Single daily doses given in the evening were more effective than the same dose given in the morning, perhaps because cholesterol is synthesized mainly at night.
In multicenter, double-blind studies in patients with familial or non-familial hypercholesterolemia, lovastatin, administered in doses ranging from 10 mg q.p.m. to 40 mg b.i.d., was compared to placebo. Lovastatin consistently and significantly decreased plasma total-C, LDL-C, total-C/HDL-C ratio and LDL-C/HDL-C ratio. In addition, lovastatin produced increases of variable magnitude in HDL-C, and modestly decreased VLDL-C and plasma TG (see
The results of a study in patients with primary hypercholesterolemia are presented in
Lovastatin was compared to cholestyramine in a randomized open parallel study. The study was performed with patients with hypercholesterolemia who were at high risk of myocardial infarction. Summary results are presented in
Lovastatin was studied in controlled trials in hypercholesterolemic patients with well-controlled non-insulin dependent diabetes mellitus with normal renal function. The effect of lovastatin on lipids and lipoproteins and the safety profile of lovastatin were similar to that demonstrated in studies in nondiabetics. Lovastatin had no clinically important effect on glycemic control or on the dose requirement of oral hypoglycemic agents.
2.1.2Expanded Clinical Evaluation of Lovastatin (EXCEL) Study
Lovastatin was compared to placebo in 8,245 patients with hypercholesterolemia (total-C 240-300 mg/dL [6.2 mmol/L-7.6 mmol/L], LDL-C >160 mg/dL [4.1 mmol/L]) in the randomized, double-blind, parallel, 48-week EXCEL study. All changes in the lipid measurements (Table IV) in lovastatin treated patients were dose-related and significantly different from placebo (p≤0.001). These results were sustained throughout the study.
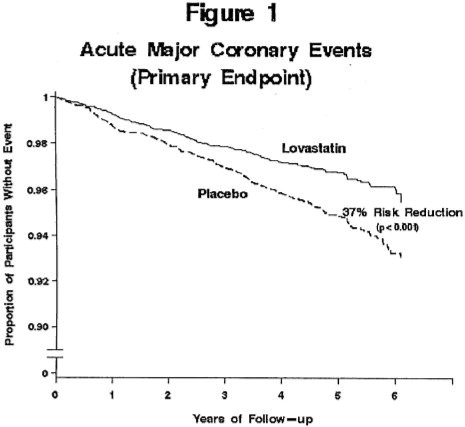
2.1.3Air Force/Texas Coronary Atherosclerosis Prevention Study (AFCAPS/TexCAPS)
The Air Force/Texas Coronary Atherosclerosis Prevention Study (AFCAPS/TexCAPS), a double-blind, randomized, placebo-controlled, primary prevention study, demonstrated that treatment with lovastatin decreased the rate of acute major coronary events (composite endpoint of myocardial infarction, unstable angina, and sudden cardiac death) compared with placebo during a median of 5.1 years of follow-up. Participants were middle-aged and elderly men (ages 45 to 73) and women (ages 55 to 73) without symptomatic cardiovascular disease with average to moderately elevated total-C and LDL-C, below average HDL-C, and who were at high risk based on elevated total-C/HDL-C. In addition to age, 63% of the participants had at least one other risk factor (baseline HDL-C <35 mg/dL, hypertension, family history, smoking and diabetes).
AFCAPS/TexCaps enrolled 6,605 participants (5,608 men, 997 women) based on the following lipid entry criteria: total-C range of 180 to 264 mg/dL, LDL-C range of 130 to 190 mg/dL, HDL-C of ≤45 mg/dL for men and ≤47 mg/dL for women, and TG of ≤400 mg/dL. Participants were treated with standard care, including diet, and either lovastatin 20 to 40 mg daily (n= 3,304) or placebo (n= 3,301). Approximately 50% of the participants treated with lovastatin were titrated to 40 mg daily when their LDL-C remained >110 mg/dL at the 20-mg starting dose.
Lovastatin reduced the risk of a first acute major coronary event, the primary efficacy endpoint, by 37% (lovastatin 3.5%, placebo 5.5%; p<0.001; Figure 1). A first acute major coronary event was defined as myocardial infarction (54 participants on lovastatin, 94 on placebo) or unstable angina (54 vs. 80) or sudden cardiac death (8 vs. 9). Furthermore, among the secondary endpoints, lovastatin reduced the risk of unstable angina by 32% (1.8 vs. 2.6%; p=0.023), of myocardial infarction by 40% (1.7 vs. 2.9%; p=0.002), and of undergoing coronary revascularization procedures (e.g., coronary artery bypass grafting or percutaneous transluminal coronary angioplasty) by 33% (3.2 vs. 4.8%; p=0.001). Trends in risk reduction associated with treatment with lovastatin were consistent across men and women, smokers and non-smokers, hypertensives and non-hypertensives, and older and younger participants. Participants with ≥2 risk factors had risk reductions (RR) in both acute major coronary events (RR 43%) and coronary revascularization procedures (RR 37%). Because there were too few events among those participants with age as their only risk factor in this study, the effect of lovastatin on outcomes could not be adequately assessed in this subgroup.
2.1.4Atherosclerosis
In the Canadian Coronary Atherosclerosis Intervention Trial (CCAIT), the effect of therapy with lovastatin on coronary atherosclerosis was assessed by coronary angiography in hyperlipidemic patients. In the randomized, double-blind, controlled clinical trial, patients were treated with conventional measures (usually diet and 325 mg of aspirin every other day) and either lovastatin 20 to 80 mg daily or placebo. Angiograms were evaluated at baseline and at two years by computerized quantitative coronary angiography (QCA). Lovastatin significantly slowed the progression of lesions as measured by the mean change per-patient in minimum lumen diameter (the primary endpoint) and percent diameter stenosis, and decreased the proportions of patients categorized with disease progression (33% vs. 50%) and with new lesions (16% vs. 32%).
In a similarly designed trial, the Monitored Atherosclerosis Regression Study (MARS), patients were treated with diet and either lovastatin 80 mg daily or placebo. No statistically significant difference between lovastatin and placebo was seen for the primary endpoint (mean change per patient in percent diameter stenosis of all lesions), or for most secondary QCA endpoints. Visual assessment by angiographers who formed a consensus opinion of overall angiographic change (Global Change Score) was also a secondary endpoint. By this endpoint, significant slowing of disease was seen, with regression in 23% of patients treated with lovastatin compared to 11% of placebo patients.
In the Familial Atherosclerosis Treatment Study (FATS), either lovastatin or niacin in combination with a bile acid sequestrant for 2.5 years in hyperlipidemic subjects significantly reduced the frequency of progression and increased the frequency of regression of coronary atherosclerotic lesions by QCA compared to diet and, in some cases, low-dose resin.
The effect of lovastatin on the progression of atherosclerosis in the coronary arteries has been corroborated by similar findings in another vasculature. In the Asymptomatic Carotid Artery Progression Study (ACAPS), the effect of therapy with lovastatin on carotid atherosclerosis was assessed by B-mode ultrasonography in hyperlipidemic patients with early carotid lesions and without known coronary heart disease at baseline. In this double-blind, controlled clinical trial, 919 patients were randomized in a 2 x 2 factorial design to placebo, lovastatin 10 to 40 mg daily and/or warfarin. Ultrasonograms of the carotid walls were used to determine the change per patient from baseline to three years in mean maximum intimal-
medial thickness (IMT) of 12 measured segments. There was a significant regression of carotid lesions in patients receiving lovastatin alone compared to those receiving placebo alone (p=0.001). The predictive value of changes in IMT for stroke has not yet been established. In the lovastatin group there was a significant reduction in the number of patients with major cardiovascular events relative to the placebo group (5 vs. 14) and a significant reduction in all-cause mortality (1 vs. 8).
2.1.5Eye
There was a high prevalence of baseline lenticular opacities in the patient population included in the early clinical trials with lovastatin. During these trials the appearance of new opacities was noted in both the lovastatin and placebo groups. There was no clinically significant change in visual acuity in the patients who had new opacities reported nor was any patient, including those with opacities noted at baseline, discontinued from therapy because of a decrease in visual acuity.
A three-year, double-blind, placebo-controlled study in hypercholesterolemic patients to assess the effect of lovastatin on the human lens demonstrated that there were no clinically or statistically significant differences between the lovastatin and placebo groups in the incidence, type or progression of lenticular opacities. There are no controlled clinical data assessing the lens available for treatment beyond three years.
3INDICATIONS AND USAGE
Therapy with lovastatin should be a component of multiple risk factor intervention in those individuals with dyslipidemia at risk for atherosclerotic vascular disease. Lovastatin should be used in addition to a diet restricted in saturated fat and cholesterol as part of a treatment strategy to lower total-C and LDL-C to target levels when the response to diet and other nonpharmacological measures alone has been inadequate to reduce risk.
3.1Primary Prevention of Coronary Heart Disease
In individuals without symptomatic cardiovascular disease, average to moderately elevated total-C and LDL-C, and below average HDL-C, lovastatin is indicated to reduce the risk of:
- Myocardial infarction
- Unstable angina
- Coronary revascularization procedures
(See
3.2Coronary Heart Disease
Lovastatin is indicated to slow the progression of coronary atherosclerosis in patients with coronary heart disease as part of a treatment strategy to lower total-C and LDL-C to target levels.
3.3Hypercholesterolemia
Therapy with lipid-altering agents should be a component of multiple risk factor intervention in those individuals at significantly increased risk for artherosclerotic vascular disease due to hypercholesterolemia. Lovastatin is indicated as an adjunct to diet for the reduction of elevated total-C and LDL-C levels in patients with primary hypercholesterolemia (Types IIa and IIb
3.4Adolescent Patients with Heterozygous Familial Hypercholesterolemia
Lovastatin is indicated as an adjunct to diet to reduce total-C, LDL-C and apolipoprotein B levels in adolescent boys and girls who are at least one year post-menarche, 10 to 17 years of age, with heFH if after an adequate trial of diet therapy the following findings are present:
- LDL-C remains >189 mg/dL or
- LDL-C remains >160 mg/dL
3.5General Recommendations
Prior to initiating therapy with lovastatin, secondary causes for hypercholesterolemia (e.g., poorly controlled diabetes mellitus, hypothyroidism, nephrotic syndrome, dysproteinemias, obstructive liver disease, other drug therapy, alcoholism) should be excluded, and a lipid profile performed to measure total-C, HDL-C, and TG. For patients with TG less than 400 mg/dL (<4.5 mmol/L), LDL-C can be estimated using the following equation:
LDL-C = total-C - [0.2 × (TG) + HDL-C]
For TG levels >400 mg/dL (>4.5 mmol/L), this equation is less accurate and LDL-C concentrations should be determined by ultracentrifugation. In hypertriglyceridemic patients, LDL-C may be low or normal despite elevated total-C. In such cases, lovastatin is not indicated.
The National Cholesterol Education Program (NCEP) Treatment Guidelines are summarized below:
After the LDL-C goal has been achieved, if the TG is still ≥200 mg/dL, non-HDL-C (total-C minus HDL-C) becomes a secondary target of therapy. Non-HDL-C goals are set 30 mg/dL higher than LDL-C goals for each risk category.
At the time of hospitalization for an acute coronary event, consideration can be given to initiating drug therapy at discharge if the LDL-C is ≥130 mg/dL (see NCEP Guidelines above).
Since the goal of treatment is to lower LDL-C, the NCEP recommends that LDL-C levels be used to initiate and assess treatment response. Only if LDL-C levels are not available, should the total-C be used to monitor therapy.
Although lovastatin may be useful to reduce elevated LDL-C levels in patients with combined hypercholesterolemia and hypertriglyceridemia where hypercholesterolemia is the major abnormality (Type IIb hyperlipoproteinemia), it has not been studied in conditions where the major abnormality is elevation of chylomicrons, VLDL or IDL (i.e., hyperlipoproteinemia types I, III, IV, or V). ***
The NCEP classification of cholesterol levels in pediatric patients with a familial history of hypercholesterolemia or premature cardiovascular disease is summarized below:
Children treated with lovastatin in adolescence should be re-evaluated in adulthood and appropriate changes made to their cholesterol-lowering regimen to achieve adult goals for LDL-C.
4CONTRAINDICATIONS
Hypersensitivity to any component of this medication.
Active liver disease or unexplained persistent elevations of serum transaminases (see
Concomitant administration with strong CYP3A4 inhibitors (e.g., itraconazole, ketoconazole, posaconazole, voriconazole, HIV protease inhibitors, boceprevir, telaprevir, erythromycin, clarithromycin, telithromycin and nefazodone) (see
5ADVERSE REACTIONS
Lovastatin is generally well tolerated; adverse reactions usually have been mild and transient.
† Manson, J.M., Freyssinges, C., Ducrocq, M.B., Stephenson, W.P., Postmarketing Surveillance of Lovastatin and Simvastatin Exposure During Pregnancy. Reproductive Toxicology. 10(6):439-446. 1996.
5.1Phase III Clinical Studies
In Phase III controlled clinical studies involving 613 patients treated with lovastatin, the adverse experience profile was similar to that shown below for the 8,245-patient EXCEL study (see
Persistent increases of serum transaminases have been noted (see
5.2Expanded Clinical Evaluation of Lovastatin (EXCEL) Study
Lovastatin was compared to placebo in 8,245 patients with hypercholesterolemia (total-C 240-300 mg/dL [6.2-7.8 mmol/L]) in the randomized, double-blind, parallel, 48-week EXCEL study. Clinical adverse experiences reported as possibly, probably or definitely drug-related in ≥1% in any treatment group are shown in the table below. For no event was the incidence on drug and placebo statistically different.
Other clinical adverse experiences reported as possibly, probably or definitely drug-related in 0.5 to 1.0 percent of patients in any drug-treated group are listed below. In all these cases the incidence on drug and placebo was not statistically different.
In the EXCEL study (see
5.3Air Force/Texas Coronary Atherosclerosis Prevention Study (AFCAPS/TexCAPS)
In AFCAPS/TexCAPS (see
5.4Concomitant Therapy
In controlled clinical studies in which lovastatin was administered concomitantly with cholestyramine, no adverse reactions peculiar to this concomitant treatment were observed. The adverse reactions that occurred were limited to those reported previously with lovastatin or cholestyramine. Other lipid-lowering agents were not administered concomitantly with lovastatin during controlled clinical studies. Preliminary data suggests that the addition of gemfibrozil to therapy with lovastatin is not associated with greater reduction in LDL-C than that achieved with lovastatin alone. In uncontrolled clinical studies, most of the patients who have developed myopathy were receiving concomitant therapy with cyclosporine, gemfibrozil or niacin (nicotinic acid). The combined use of lovastatin with cyclosporine or gemfibrozil should be avoided. Caution should be used when prescribing other fibrates or lipid-lowering doses (≥1 g/day) of niacin with lovastatin (see
The following effects have been reported with drugs in this class. Not all the effects listed below have necessarily been associated with lovastatin therapy.
Skeletal: muscle cramps, myalgia, myopathy, rhabdomyolysis, arthralgias.
There have been rare reports of immune-mediated necrotizing myopathy associated with statin use [see
Neurological: dysfunction of certain cranial nerves (including alteration of taste, impairment of extra-ocular movement, facial paresis), tremor, dizziness, vertigo, paresthesia, peripheral neuropathy, peripheral nerve palsy, psychic disturbances, anxiety, insomnia, depression.
There have been rare postmarketing reports of cognitive impairment (e.g., memory loss, forgetfulness, amnesia, memory impairment, confusion) associated with statin use. These cognitive issues have been reported for all statins. The reports are generally nonserious, and reversible upon statin discontinuation, with variable times to symptom onset (1 day to years) and symptom resolution (median of 3 weeks).
Hypersensitivity Reactions: An apparent hypersensitivity syndrome has been reported rarely which has included one or more of the following features: anaphylaxis, angioedema, lupus erythematous-like syndrome, polymyalgia rheumatica, dermatomyositis, vasculitis, purpura, thrombocytopenia, leukopenia, hemolytic anemia, positive ANA, ESR increase, eosinophilia, arthritis, arthralgia, urticaria, asthenia, photosensitivity, fever, chills, flushing, malaise, dyspnea, toxic epidermal necrolysis, erythema multiforme, including Stevens-Johnson syndrome.
Gastrointestinal: pancreatitis, hepatitis, including chronic active hepatitis, cholestatic jaundice, fatty change in liver; and rarely, cirrhosis, fulminant hepatic necrosis, and hepatoma; anorexia, vomiting, fatal and non-fatal hepatic failure.
Skin: alopecia, pruritus. A variety of skin changes (e.g., nodules, discoloration, dryness of skin/mucous membranes, changes to hair/nails) have been reported.
Reproductive: gynecomastia, loss of libido, erectile dysfunction.
Eye: progression of cataracts (lens opacities), ophthalmoplegia.
Laboratory Abnormalities: elevated transaminases, alkaline phosphatase, γ-glutamyl transpeptidase, and bilirubin; thyroid function abnormalities.
5.5Adolescent Patients (ages 10 to 17 years)
In a 48-week controlled study in adolescent boys with heFH (n=132) and a 24-week controlled study in girls who were at least 1 year post-menarche with heFH (n=54), the safety and tolerability profile of the groups treated with lovastatin (10 to 40 mg daily) was generally similar to that of the groups treated with placebo (see
6OVERDOSAGE
After oral administration of lovastatin to mice, the median lethal dose observed was >15 g/m
Five healthy human volunteers have received up to 200 mg of lovastatin as a single dose without clinically significant adverse experiences. A few cases of accidental overdosage have been reported; no patients had any specific symptoms, and all patients recovered without sequelae. The maximum dose taken was 5 to 6 g.
Until further experience is obtained, no specific treatment of overdosage with lovastatin can be recommended.
The dialyzability of lovastatin and its metabolites in man is not known at present.
7DOSAGE AND ADMINISTRATION
The patient should be placed on a standard cholesterol-lowering diet before receiving lovastatin and should continue on this diet during treatment with lovastatin (see NCEP Treatment Guidelines for details on dietary therapy). Lovastatin should be given with meals.
7.1Adult Patients
The usual recommended starting dose is 20 mg once a day given with the evening meal. The recommended dosing range is 10 to 80 mg/day in single or two divided doses; the maximum recommended dose is 80 mg/day. Doses should be individualized according to the recommended goal of therapy (see NCEP Guidelines and
Cholesterol levels should be monitored periodically and consideration should be given to reducing the dosage of lovastatin if cholesterol levels fall significantly below the targeted range.
8Dosage in Patients taking Danazol, Diltiazem, Dronedarone, or Verapamil
In patients taking danazol, diltiazem, dronedarone or verapamil concomitantly with lovastatin, therapy should begin with 10 mg of lovastatin and should not exceed 20 mg
8.1Dosage in Patients taking Amiodarone
In patients taking amiodarone concomitantly with lovastatin, the dose should not exceed 40 mg/day (see
8.2Adolescent Patients (10 to 17 years of age) with Heterozygous Familial Hypercholesterolemia
The recommended dosing range is 10 to 40 mg/day; the maximum recommended dose is 40 mg/day. Doses should be individualized according to the recommended goal of therapy (see NCEP Pediatric Panel Guidelines ††,
8.3Concomitant Lipid-Lowering Therapy
Lovastatin is effective alone or when used concomitantly with bile-acid sequestrants (see
8.4Dosage in Patients with Renal Insufficiency
In patients with severe renal insufficiency (creatinine clearance <30 mL/min), dosage increases above 20 mg/day should be carefully considered and, if deemed necessary, implemented cautiously (see
9HOW SUPPLIED
Lovastatin Tablets USP (white to off white round, unscored tablets) containing 40mg of lovastatin and engraved with “CTI”
143 ----Bottle of 30 (NDC 63187-345-30)
143 ----Bottle of 60 (NDC 63187-345-60)
143 ----Bottle of 90 (NDC 63187-345-90)
†† National Cholesterol Education Program (NCEP): Highlights of the Report of the Expert Panel on Blood Cholesterol Levels in Children and Adolescents. Pediatrics . 89(3):495-501, 1992.
9.1Storage
Store at 20º to 25º C (68º to 77º F). [See USP Controlled Room Temperature.] Lovastatin Tablets must be protected from light and stored in a well-closed, light-resistant container.
Manufactured and Distributed By:
Repackaged by:
Revised May 2013