Generic Name
Ethynodiol
Brand Names
Kelnor, Valtya, Zovia
FDA approval date: June 20, 2005
Form: Kit
What is Kelnor (Ethynodiol)?
Kelnor 1/35 is indicated for the prevention of pregnancy in women who elect to use oral contraceptives as a method of contraception. Oral contraceptives are highly effective. Table 1 lists the typical accidental pregnancy rates for users of combination oral contraceptives and other methods of contraception. The efficacy of these contraceptive methods, except sterilization and progestogen implants and injections, depends upon the reliability with which they are used. Correct and consistent use of methods can result in lower failure rates. TABLE 1: PERCENTAGE OF WOMEN EXPERIENCING AN UNINTENDED PREGNANCY DURING THE FIRST YEAR OF TYPICAL USE AND THE FIRST YEAR OF PERFECT USE OF CONTRACEPTION AND THE PERCENTAGE CONTINUING USE AT THE END OF THE FIRST YEAR. UNITED STATES. % of Women Experiencing an Unintended Pregnancy Within the First Year of Use % of Women Continuing Use at One Year 1 Method Typical Use 2 Perfect Use 3 Chance 4 85 85 Spermicides 5 26 6 40 Periodic abstinence 25 63 Calendar 9 Ovulation method 3 Sympto-thermal 6 2 Post-ovulation 1 Withdrawal 19 4 Cap 7 Parous women 40 26 42 Nulliparous women 20 9 56 Sponge Parous women 40 20 42 Nulliparous women 20 9 56 Diaphragm 7 20 6 56 Condom 8 Female 21 5 56 Male 14 3 61 Pill 5 71 Progestin only.
Approved To Treat
Top Global Experts
There are no experts for this drug
Save this treatment for later
Not sure about your diagnosis?
Related Clinical Trials
There is no clinical trials being done for this treatment
Related Latest Advances
Brand Information
Kelnor 1/35 (Ethynodiol Diacetate and Ethinyl Estradiol)
1DESCRIPTION
Kelnor
The chemical name for ethynodiol diacetate, USP is 19-nor-17α-pregn-4-en-20-yne-3β, 17-diol diacetate, and for ethinyl estradiol, USP it is 19-nor-17α-pregna-1, 3, 5 (10)-trien-20-yne-3, 17-diol. The structural formulas are as follows:
Ethynodiol Diacetate, USP
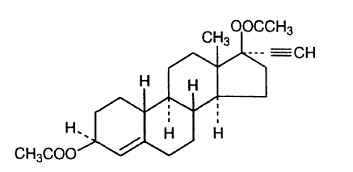
C
Ethinyl Estradiol, USP
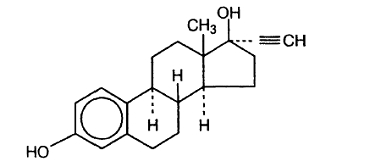
C
2CLINICAL PHARMACOLOGY
Combination oral contraceptives act primarily by suppression of gonadotropins. Although the primary mechanism of this action is inhibition of ovulation, other alterations in the genital tract, including changes in the cervical mucus (which increase the difficulty of sperm entry into the uterus) and the endometrium (which may reduce the likelihood of implantation) may also contribute to contraceptive effectiveness.
3INDICATIONS AND USAGE
Kelnor 1/35 (28 Day Regimen) (ethynodiol diacetate and ethinyl estradiol tablets) is indicated for the prevention of pregnancy in women who elect to use oral contraceptives as a method of contraception.
Oral contraceptives are highly effective.
TABLE 1: PERCENTAGE OF WOMEN EXPERIENCING AN UNINTENDED PREGNANCY DURING THE FIRST YEAR OF TYPICAL USE AND THE FIRST YEAR OF PERFECT USE OF CONTRACEPTION AND THE PERCENTAGE CONTINUING USE AT THE END OF THE FIRST YEAR. UNITED STATES.
1. Among couples attempting to avoid pregnancy, the percentage who continue to use a method for one year.
2. Among typical couples who initiate use of a method (not necessarily for the first time), the percentage who experience an accidental pregnancy during the first year if they do not stop use for any other reason.
3. Among couples who initiate use of a method (not necessarily for the first time) and who use it perfectly (both consistently and correctly), the percentage who experience an accidental pregnancy during the first year if they do not stop use for any other reason.
4. The percents becoming pregnant in columns (2) and (3) are based on data from populations where contraception is not used and from women who cease using contraception in order to become pregnant. Among such populations, about 89% become pregnant within one year. This estimate was lowered slightly (to 85%) to represent the percent who would become pregnant within one year among women now relying on reversible methods of contraception if they abandoned contraception altogether.
5. Foams, creams, gels, vaginal suppositories, and vaginal film.
6. Cervical mucus (ovulation) method supplemented by calendar in the pre-ovulatory and basal body temperature in the post-ovulatory phases.
7. With spermicidal cream or jelly.
8. Without spermicides.
9. The treatment schedule is one dose within 72 hours after unprotected intercourse, and a second dose 12 hours after the first dose. The Food and Drug Administration has declared the following brands of oral contraceptives to be safe and effective for emergency contraception: Ovral® (1 dose is 2 white pills), Alesse® (1 dose is 5 pink pills), Nordette® or Levlen® (1 dose is 2 light-orange pills), Lo/Ovral® (1 dose is 4 white pills), Triphasil® or Tri-Levlen® (1 dose is 4 yellow pills).
4CONTRAINDICATIONS
Kelnor 1/35 is contraindicated in females who are known to have or develop the following conditions:
- Thrombophlebitis or thromboembolic disorders
- A past history of deep vein thrombophlebitis or thromboembolic disorders
- Cerebral vascular disease, myocardial infarction, or coronary artery disease, or a past history of these conditions
- Current diagnosis of, or history of, breast cancer, which may be hormone-sensitive
- Known or suspected carcinoma of the female reproductive organs or suspected estrogen-dependent neoplasia, or a history of these conditions
- Undiagnosed abnormal genital bleeding
- History of cholestatic jaundice of pregnancy or jaundice with prior oral contraceptive use
- Past or present, benign or malignant liver tumors
- Known or suspected pregnancy
- Are receiving Hepatitis C drug combinations containing ombitasvir/paritaprevir/ritonavir, with or without dasabuvir, due to the potential for ALT elevations (see WARNINGS,
5WARNINGS
The use of oral contraceptives is associated with increased risk of several serious conditions including venous and arterial thromboembolism, thrombotic and hemorrhagic stroke, myocardial infarction, liver tumors or other liver lesions, and gallbladder disease. The risk of morbidity and mortality increases significantly in the presence of other risk factors such as hypertension, hyperlipidemia, obesity, and diabetes mellitus.
Practitioners prescribing oral contraceptives should be familiar with the following information relating to these and other risks.
The information contained herein is principally based on studies carried out in patients who used oral contraceptives with formulations containing higher amounts of estrogens and progestogens than those in common use today. The effect of long-term use of the oral contraceptives with lesser amounts of both estrogens and progestogens remains to be determined.
Throughout this labeling, epidemiological studies reported are of two types: retrospective case-control studies and prospective cohort studies. Case-control studies provide an estimate of the relative risk of a disease, which is defined as the
5.1Estimates of Mortality From Contraceptive Use
One study
Because of these changes in practice and, also, because of some limited new data that suggest that the risk of cardiovascular disease with the use of oral contraceptives may now be less than previously observed,
Therefore, the Committee recommended that the benefits of oral contraceptive use by healthy nonsmoking women over 40 may outweigh the possible risks. Of course, older women, as all women who take oral contraceptives, should take the lowest possible dose formulation that is effective.
TABLE 2: ANNUAL NUMBER OF BIRTH-RELATED OR METHOD-RELATED DEATHS ASSOCIATED WITH CONTROL OF FERTILITY PER 100,000 NONSTERILE WOMEN, BY FERTILITY CONTROL METHOD ACCORDING TO AGE.
1. Deaths are birth-related
2. Deaths are method-related
Adapted from Ory.
5.2Malignant Neoplasms
Breast Cancer
Kelnor is contraindicated in females who currently have or have had breast cancer because breast cancer may be hormonally sensitive [see
Epidemiology studies have not found a consistent association between use of combined oral contraceptives (COCs) and breast cancer risk. Studies do not show an association between ever (current or past) use of COCs and risk of breast cancer. However, some studies report a small increase in the risk of breast cancer among current or recent users (<6 months since last use) and current users with longer duration of COC use [see
Cervical Cancer
Some studies suggested that oral contraceptive use was associated with an increase in the risk of cervical intraepithelial neoplasia, dysplasia, erosion, carcinoma, or microglandular dysplasia in some populations of women.
In spite of many studies of the relationship between oral contraceptive use and breast and cervical cancers, a cause and effect relationship has not been established.
5.3Hepatic Neoplasia
Benign hepatic adenomas and other hepatic lesions have been associated with oral contraceptive use,
Studies from the U.S.,
5.4Risk of Liver Enzyme Elevations with Concomitant Hepatitis C Treatment
During clinical trials with the Hepatitis C combination drug regimen that contains ombitasvir/paritaprevir/ritonavir, with or without dasabuvir, ALT elevations greater than 5 times the upper limit of normal (ULN), including some cases greater than 20 times the ULN, were significantly more frequent in women using ethinyl estradiol-containing medications such as COCs. Discontinue Kelnor prior to starting therapy with the combination drug regimen ombitasvir/paritaprevir/ritonavir, with or without dasabuvir (see
5.5Ocular Lesions
There have been reports of retinal thrombosis and other ocular lesions associated with the use of oral contraceptives. Oral contraceptives should be discontinued if there is unexplained, gradual or sudden, partial or complete loss of vision; onset of proptosis or diplopia; papilledema; or any evidence of retinal vascular lesions. Appropriate diagnostic and therapeutic measures should be undertaken immediately.
5.6Oral Contraceptive Use Before or During Pregnancy
Extensive epidemiological studies have revealed no increased risk of birth defects in women who have used oral contraceptives prior to pregnancy.
The administration of oral contraceptives to induce withdrawal bleeding should not be used as a test for pregnancy. Oral contraceptives should not be used during pregnancy to treat threatened or habitual abortion. It is recommended that for any patient who has missed two consecutive periods, pregnancy should be ruled out before continuing oral contraceptive use. If the patient has not adhered to the prescribed schedule, the possibility of pregnancy should be considered at the time of the first missed period and further use of oral contraceptives should be withheld until pregnancy has been ruled out. Oral contraceptive use should be discontinued if pregnancy is confirmed.
5.7Gallbladder Disease
Earlier studies reported an increased lifetime relative risk of gallbladder surgery in users of oral contraceptives and estrogens.
5.8Carbohydrate and Lipid Metabolic Effects
Oral contraceptives have been shown to cause a decrease in glucose tolerance in a significant percentage of users.
Some women may have persistent hypertriglyceridemia while on the pill. As discussed earlier (see
5.9Elevated Blood Pressure
An increase in blood pressure has been reported in women taking oral contraceptives
Women with a history of hypertension or hypertension-related disease, or renal disease
5.10Headache
The onset or exacerbation of migraine or the development of headache of a new pattern that is recurrent, persistent, or severe requires discontinuation of oral contraceptives and evaluation of the cause.
5.11Bleeding Irregularities
Breakthrough bleeding and spotting are sometimes encountered in patients on oral contraceptives, especially during the first three months of use. Nonhormonal causes should be considered and adequate diagnostic measures taken to rule out malignancy or pregnancy in the event of breakthrough bleeding, as in the case of any abnormal vaginal bleeding. If a pathologic basis has been excluded, time alone or a change to another formulation may solve the problem. In the event of amenorrhea, pregnancy should be ruled out. Some women may encounter post-pill amenorrhea or oligomenorrhea, especially when such a condition was pre-existent.
6INFORMATION FOR THE PATIENT
See patient labeling printed below.
7ADVERSE REACTIONS
Post Marketing Experience
Five studies that compared breast cancer risk between ever-users (current or past use) of COCs and never-users of COCs reported no association between ever use of COCs and breast cancer risk, with effect estimates ranging from 0.90 - 1.12 (
Three studies compared breast cancer risk between current or recent COC users (<6 months since last use) and never users of COCs (
Figure 2: Risk of Breast Cancer with Combined Oral Contraceptive Use
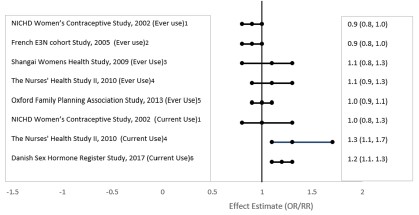
RR = relative risk; OR = odds ratio; HR = hazard ratio. “ever COC” are females with current or past COC use; “never COC use” are females that never used COCs.
An increased risk of the following serious adverse reactions has been associated with the use of oral contraceptives (see
- Thrombophlebitis and thrombosis
- Arterial thromboembolism
- Pulmonary embolism
- Myocardial infarction and coronary thrombosis
- Cerebral hemorrhage
- Cerebral thrombosis
- Hypertension
- Gallbladder disease
- Benign and malignant liver tumors, and other hepatic lesions
There is evidence of an association between the following conditions and the use of oral contraceptives, although additional confirmatory studies are needed:
- Mesenteric thrombosis
- Neuro-ocular lesions (e.g., retinal thrombosis and optic neuritis)
The following adverse reactions have been reported in patients receiving oral contraceptives and are believed to be drug-related:
- Nausea
- Vomiting
- Gastrointestinal symptoms (such as abdominal cramps and bloating)
- Breakthrough bleeding
- Spotting
- Change in menstrual flow
- Amenorrhea during or after use
- Temporary infertility after discontinuation of use
- Edema
- Chloasma or melasma, which may persist
- Breast changes: tenderness, enlargement, secretion
- Change in weight (increase or decrease)
- Change in cervical erosion or secretion
- Diminution in lactation when given immediately postpartum
- Cholestatic jaundice
- Migraine
- Rash (allergic)
- Mental depression
- Reduced tolerance to carbohydrates
- Vaginal candidiasis
- Change in corneal curvature (steepening)
- Intolerance to contact lenses
The following adverse reactions or conditions have been reported in users of oral contraceptives and the association has been neither confirmed nor refuted:
- Premenstrual syndrome
- Cataracts
- Changes in appetite
- Cystitis-like syndrome
- Headache
- Nervousness
- Dizziness
- Hirsutism
- Loss of scalp hair
- Erythema multiforme
- Erythema nodosum
- Hemorrhagic eruption
- Vaginitis
- Porphyria
- Impaired renal function
- Hemolytic uremic syndrome
- Acne
- Changes in libido
- Colitis
- Budd-Chiari syndrome
- Endocervical hyperplasia or ectropion
8OVERDOSAGE
Serious ill effects have not been reported following acute ingestion of large doses of oral contraceptives by young children.
9NON-CONTRACEPTIVE HEALTH BENEFITS
The following non-contraceptive health benefits related to the use of oral contraceptives are supported by epidemiological studies that largely utilized oral contraceptive formulations containing estrogen doses exceeding 35 mcg of ethinyl estradiol or 50 mcg of mestranol.
Effects on Menses
- Increased menstrual cycle regularity
- Decreased blood loss and decreased risk of iron-deficiency anemia
- Decreased frequency of dysmenorrhea
Effects Related to Inhibition of Ovulation
- Decreased risk of functional ovarian cysts
- Decreased risk of ectopic pregnancies
Effects From Long-Term Use
- Decreased risk of fibroadenomas and fibrocystic disease of the breast
- Decreased risk of acute pelvic inflammatory disease
- Decreased risk of endometrial cancer
- Decreased risk of ovarian cancer
- Decreased risk of uterine fibroids
10DOSAGE AND ADMINISTRATION
To achieve maximum contraceptive effectiveness, oral contraceptives must be taken exactly as directed and at intervals of 24 hours.
IMPORTANT: If the Sunday start schedule is selected, the patient should be instructed to use an additional method of protection until after the first week of administration
Kelnor 1/35 (28 Day Regimen) (ethynodiol diacetate and ethinyl estradiol tablets)
10.1Dosage Schedule
The Kelnor 1/35 (28 Day Regimen) tablet dispenser contains 21 light yellow active tablets arranged in three numbered rows of 7 tablets each, followed by a fourth row of 7 white placebo tablets.
Days of the week are printed above the tablets, starting with Sunday on the left.
10.2Day Schedule
For a DAY 1 START, count the first day of menstrual flow as Day 1 and the first tablet (light yellow) is then taken on Day 1. For a SUNDAY START when menstrual flow begins on or before Sunday, the first tablet (light yellow) is taken on that day. With either a DAY 1 START or SUNDAY START, 1 tablet (light yellow) is taken each day at the same time for 21 days. Then the white tablets are taken for 7 days, whether bleeding has stopped or not. After all 28 tablets have been taken, whether bleeding has stopped or not, the same dosage schedule is repeated beginning on the following day.
11HOW SUPPLIED
Kelnor
Store at 20° to 25°C (68° to 77°F) [See USP Controlled Room Temperature].
KEEP THIS AND ALL MEDICATIONS OUT OF THE REACH OF CHILDREN.
12REFERENCES
1. Hatcher RA, et al. Contraceptive Technology: Seventeenth Revised Edition. New York, NY, 1998. 1a. Physicians' Desk Reference. 47th ed. Oradell, NJ: Medical Economics Co Inc; 1993:2598-2601. 2. Mann JI, et al. Br Med J. 1975;2(May 3):241. 3. Mann JI, et al. Br Med J. 1975;3(Sept 13):631. 4. Mann JI, et al. Br Med J. 1975;2(May 3):245. 5. Mann JI, et al. Br Med J. 1976;2(Aug 21):445. 6. Arthes FG, et al. Chest. 1976;70(Nov):574. 7. Jain AK, Am J Obstet Gynecol. 1976;301(Oct 1):126; and Stud Fam Plann. 1977;8(March):50. 8. Ory HW. JAMA. 1977;237(June 13):2619. 9. Jick H, et al. JAMA. 1978;239(April 3):1403, 1407. 10. Jick H, et al. JAMA. 1978;240(Dec 1):2548. 11. Shapiro S, et al. Lancet. 1979;1(April 7):743. 12. Rosenberg L, et al. Am J Epidemiol. 1980;111(Jan):59. 13. Krueger DE, et al. Am J Epidemiol. 1980;111(June):655. 14. Layde P, et al. Lancet. 1981;1(March 7):541. 15. Adam SA, et al. Br J Obstet Gynaecol. 1981;88(Aug):838. 16. Slone D, et al. N Engl J Med. 1981;305(Aug 20):420. 17. Ramcharan S, et al. The Walnut Creek Contraceptive Drug Study. Vol 3. US Govt Ptg Off; 1981; and J Reprod Med. 1980;25(Dec):346. 18. Layde PM, et al. J R Coll Gen Pract. 1983;33(Feb):75. 19. Rosenberg L, et al. JAMA. 1985;253(May 24/31):2965. 20. Mant D, et al. J Epidemiol Community Health. 1987;41(Sept):215. 21. Croft P, et al. Br Med J. 1989;298(Jan 21):165. 22. Goldbaum GM, et al. JAMA. 1987;258(Sept 11):1339. 23. Bradley DD, et al. N Engl J Med. 1978;299(July 6):17. 24. Tikkanen MJ. J Reprod Med. 1986;31(Sept suppl):898. 25. Lipson A, et al. Contraception. 1986;34(Aug):121. 26. Burkman RT, et al. Obstet Gynecol. 1988; 71(Jan):33. 27. Knopp RH, J Reprod Med. 1986;31(Sept suppl):913. 28. Krauss RM, et al. Am J Obstet Gynecol. 1983;145(Feb 15):446. 29. Wahl P, et al. N Engl J Med. 1983;308(April 14):862. 30. Wynn V, et al. Am J Obstet Gynecol. 1982;142(March 15):766. 31. LaRosa JC. J Reprod Med. 1986;31(Sept suppl):906. 32. Wynn V, et al. J Reprod Med. 1986;31(Sept suppl):892. 33. Royal College of General Practitioners. J R Coll Gen Pract. 1967;13(May):267. 34. Inman WHW, et al. Br Med J. 1968;2(April 27):193. 35. Vessey MP, et al. Br Med J. 1968;2(April 27):199. 36. Vessey MP, et al. Br Med J. 1969;2(June 14):651. 37. Sartwell PE, et al. Am J Epidemiol. 1969;90(Nov):365. 38. Vessey MP, et al. Br Med J. 1970;3(July 18):123. 39. Greene GR, et al. Am J Public Health. 1972;62(May):680. 40. Boston Collaborative Drug Surveillance Programme. Lancet. 1973;1(June 23):1399. 41. Stolley PD, et al. Am J Epidemiol. 1975;102(Sept):197. 42. Vessey MP, et al. J Biosoc Sci. 1976;8(Oct):373. 43. Kay CR, J R Coll Gen Pract. 1978;28(July):393. 44. Petitti DB, et al. Am J Epidemiol. 1978;108(Dec):480. 45. Maguire MG, et al. Am J Epidemiol. 1979;110(Aug):188. 46. Petitti DB, et al. JAMA. 1979;242(Sept 14):1150. 47. Porter JB, et al. Obstet Gynecol. 1982;59(March):299. 48. Porter JB, et al. Obstet Gynecol. 1985;66(July):1. 49. Vessey MP, et al. Br Med J. 1986;292(Feb 22):526. 50. Hoover R, et al. Am J Public Health. 1978;68(April):335. 51. Vessey MP. Br J Fam Plann. 1980;6(Oct suppl):1. 52. Collaborative Group for the Study of Stroke in Young Women. N Engl J Med. 1973;288(April 26):871. 53. Royal College of General Practitioners. Oral Contraceptives and Health. New York, NY: Pitman Publ Corp; May 1974. 54. Collaborative Group for the Study of Stroke in Young Women. JAMA. 1975;231(Feb 17):718. 55. Beral V. Lancet. 1976;2(Nov 13):1047. 56. Vessey MP, et al. Lancet. 1977;2(Oct 8):731; and 1981;1(March 7):549. 57. Petitti DB, et al. Lancet. 1978;2(July 29):234. 58. Inman WHW. Br Med J. 1979;2(Dec 8):1468. 59. Vessey MP, et al. Br Med J. 1984;289(Sept 1):530. 60. Inman WHW, et al. Br Med J. 1970;2(April 25):203. 61. Meade TW, et al. Br Med J. 1980;280(May 10):1157. 62. Böttiger LE, et al. Lancet. 1980;1(May 24):1097. 63. Kay CR, Am J Obstet Gynecol. 1982;142(March 15):762. 64. Vessey MP, et al. Br Med J. 1986;292(Feb 22):526. 65. Gordon T, et al. Am J Med. 1977;62(May):707. 66. Beral V, et al. Lancet. 1977;2(Oct 8):727. 67. Ory H. Fam Plann Perspect. 1983;15(March-April):57. 68. Arthes FG, et al. Cancer. 1971;28(Dec):1391. 69. Vessey MP, et al. Br Med J. 1972;3(Sept 23):719. 70. Boston Collaborative Drug Surveillance Program. N Engl J Med. 1974;290(Jan 3):15. 71. Vessey MP, et al. Lancet. 1975;1(April 26):941. 72. Casagrande J, et al. J Natl Cancer Inst. 1976;56(April):839. 73. Kelsey JL, et al. Am J Epidemiol. 1978;107(March):236. 74. Kay CR. Br Med J. 1981;282(June 27):2089. 75. Vessey MP, et al. Br Med J. 1981;282(June 27):2093. 76. The Cancer and Steroid Hormone Study of the Center for Disease Control and the National Institute of Child Health and Human Development. Oral contraceptive use and the risk of breast cancer. N Engl J Med. 1986;315(Aug 14):405. 77. Paul C, et al. Br Med J. 1986; 293(Sept 20):723. 78. Miller DR, et al. Obstet Gynecol. 1986;68(Dec):863. 79. Pike MC, et al. Lancet. 1983;2(Oct 22):926. 80. McPherson K, et al. Br J Cancer. 1987;56(Nov):653. 81. Hoover R, et al. N Engl J Med. 1976;295(Aug 19):401. 82. Lees AW, et al. Int J Cancer. 1978;22(Dec):700. 83. Brinton LA, et al. J Natl Cancer Inst. 1979;62(Jan):37. 84. Black MM, Pathol Res Pract. 1980;166:491; and Cancer. 1980;46(Dec):2747; and Cancer. 1983;51(June):2147. 85. Thomas DB. JNCI. 1993;85(March 3):359. 86. Brinton LA, et al. Int J Epidemiol. 1982;11(Dec):316. 87. Harris NV, et al. Am J Epidemiol. 1982;116(Oct):643. 88. Jick H, et al. Am J Epidemiol. 1980;112(Nov):577. 89. McPherson K, et al. Lancet. 1983;2(Dec 17):1414. 90. Hoover R, et al. J Natl Cancer Inst. 1981;67(Oct):815. 91. Jick H, et al. Am J Epidemiol. 1980;112(Nov):586. 92. Meirik O, et al. Lancet. 1986;2(Sept 20):650. 93. Fasal E, et al. J Natl Cancer Inst. 1975;55(Oct):767. 94. Paffenbarger RS, et al. Cancer. 1977;39(April suppl):1887. 95. Stadel BV, et al. Contraception. 1988;38(Sept):287. 96. Miller DR, et al. Am J Epidemiol. 1989;129(Feb):269. 97. Kay CR, et al. Br J Cancer. 1988;58(Nov):675. 98. Miller DR, et al. Obstet Gynecol. 1986;68(Dec):863. 99. Hulka BS, et al. Cancer. 1994;74(August 1 suppl):1111. 100. Chilvers C, et al. Lancet. 1989;1(May 6):973. 101. Huggins GR, et al. Fertil Steril. 1987;47(May):733. 102. Pike MC, et al. Br J Cancer. 1981;43(Jan):72. 103. Ory H, et al. Am J Obstet Gynecol. 1976;124(March 15):573. 104. Stern E, et al. Science. 1977;196(June 24):1460. 105. Peritz E, et al. Am J Epidemiol. 1977;106(Dec):462. 106. Ory HW, et al. In: Garattini S, Berendes H, eds. Pharmacology of Steroid Contraceptive Drugs. New York, NY: Raven Press; 1977;211-224. 107. Meisels A, et al. Cancer. 1977;40(Dec):3076. 108. Goldacre MJ, et al. Br Med J. 1978;1(March 25):748. 109. Swan SH, et al. Am J Obstet Gynecol. 1981;139(Jan 1):52. 110. Vessey MP, et al. Lancet. 1983;2(Oct 22):930. 111. Dallenbach-Hellweg G. Pathol Res Pract. 1984;179:38. 112. Thomas DB, et al. Br Med J. 1985;290(March 30):961. 113. Brinton LA, et al. Int J Cancer. 1986;38 (Sept):339. 114. Ebeling K, et al. Int J Cancer. 1987;39(April):427. 115. Beral V, et al. Lancet. 1988;2(Dec 10):1331. 116. Baum JK, et al. Lancet. 1973;2(Oct 27):926. 117. Edmondson HA, et al. N Engl J Med. 1976;294(Feb 26):470. 118. Bein NN, et al. Br J Surg. 1977;64(June):433. 119. Klatskin G. Gastroenterology. 1977;73(Aug):386. 120. Rooks JB, et al. JAMA. 1979;242(Aug 17):644. 121. Sturtevant FM. In: Moghissi K, ed. Controversies in Contraception. Baltimore, MD: Williams & Wilkins; 1979:93-150. 122. Henderson BE, et al. Br J Cancer. 1983;48(July):437. 123. Neuberger J, et al. Br Med J. 1986;292(May 24):1355. 124. Forman D, et al. Br Med J. 1986;292(May 24):1357. 125. La Vecchia C, et al. Br J Cancer. 1989;59(March):460. 126. Savolainen E, et al. Am J Obstet Gynecol. 1981;140(July 1):521. 127. Ferencz C, et al. Teratology. 1980;21(April):225. 128. Rothman KJ, et al. Am J Epidemiol. 1979;109(April):433. 129. Harlap S, et al. Obstet Gynecol. 1980;55(April):447. 130. Layde PM, et al. J Epidemiol Community Health. 1982;36(Dec):274. 131. Rome Group for the Epidemiology and Prevention of Cholelithiasis (GREPCO). Am J Epidemiol. 1984;119(May):796. 132. Strom BL, et al. Clin Pharmacol Ther. 1986;39(March):335. 133. Wynn V. In: Bardin CE, et al. eds. Progesterone and Progestins. New York, NY: Raven Press;1983:395-410. 134. Perlman JA, et al. J Chron Dis. 1985;38(Oct)857. 135. Powell MG, et al. Obstet Gynecol. 1984;63(June):764. 136. Wynn V, et al. Lancet. 1966;2(Oct 1):720. 137. Fisch IR, et al. JAMA. 1977;237(June 6):2499. 138. Kay CR. Lancet. 1977;1(March 19):624. 139. Laragh JH. Am J Obstet Gynecol. 1976;126(Sept 1):141. 140. Ramcharan S. In: Garattini S, Berendes HW, eds. Pharmacology of Steroid Contraceptive Drugs. New York, NY: Raven Press; 1977:277-288. 141. Laumas KR, et al. Am J Obstet Gynecol. 1967;98(June 1):411. 142. Saxena BN, et al. Contraception. 1977;16(Dec):605. 143. Nilsson S. et al. Contraception. 1978;17(Feb):131. 144. Washington AE, et al. JAMA. 1985;253(April 19):2246. 145. Louv WC, et al. Am J Obstet Gynecol. 1989;160(Feb):396. 146. Francis WG, et al. Can Med Assoc J. 1965;92(Jan 23):191. 147. Verhulst HL, et al. J Clin Pharmacol. 1967;7(Jan-Feb):9. 148. Ory HW. Fam Plann Perspect. 1982;14(July-Aug):182. 149. Ory HW, et al. Making Choices: Evaluating the Health Risks and Benefits of Birth Control Methods. New York, NY: The Alan Guttmacher Institute; 1983. 150. Palmer JR, et al. Am J Epidemiol. 1989;130(Nov):878. 151. Romieu I, et al. J Natl Cancer Inst. 1989;81(Sept):1313. 152. Porter JB, et al. Obstet Gynecol. 1987;70(July):29. 153. Olsson H, et al. Cancer Detect Prev. 1991;15:265. 154. Delgado-Rodriguez M, et al. Rev Epidém Santé Publ. 1991;39:165. 155. Clavel F, et al. Int J Epidemiol. 1991;20(March):32. 156. Brinton LA, et al. JNCI. 1995;87(June 7):827. 157. Thomas DB, et al. Br J Cancer. 1992;65(January):108. 158. Thomas DB, et al. Cancer Causes Cont. 1991;2(Nov):389. 159. Weinstein AL, et al. Epidemiology. 1991;2(Sept):353. 160. Ranstam J, et al. Anticancer Res. 1991;11(Nov-Dec):2043. 161. Ursin G, et al. Epidemiology. 1992;3(Sept):414. 162. White E, et al. JNCI. 1994;86(April 6):505. 163. Mann R, et al. Oral Contraceptives and Breast Cancer. Park Ridge, NJ: The Parthenon Publishing Group Inc.; 1990. 164. Institute of Medicine. Committee on the Relationship Between Oral Contraceptives and Breast Cancer. Oral Contraceptives and Breast Cancer. Washington, DC: National Academy Press; 1991. 165. Harlap S. J Reprod Med. 1991;36(May):374. 166. Rushton L, et al. Br J Obstet Gynaecol. 1992;99(March):239. 167. Colditz G. Cancer. 1993;71(Feb 15 suppl):1480.
TEVA PHARMACEUTICALS USA, INC.North Wales, PA 19454
Rev. E 10/2022
13BRIEF SUMMARY OF PATIENT WARNINGS
This product (like all oral contraceptives) is intended to prevent pregnancy. It does not protect against HIV infection (AIDS) and other sexually transmitted diseases.
14Package/Label Display Panel, Part 1 of 2
NDC 0555-9064-58
6 Blister Card Dispensers, 28 Tablets Each
28
DAY
REGIMEN
Kelnor® 1/35
(ethynodiol diacetate and
ethinyl estradiol tablets USP)
Contains 6 blister cards, each containing 28 tablets. Each light yellow
tablet contains 1 mg ethynodiol diacetate, USP and 35 mcg ethinyl
estradiol, USP. Each white tablet contains inert ingredients.
Rx only
SHAPING
WOMEN’S HEALTH®
15Package/Label Display Panel, Part 2 of 2