Generic Name
Sildenafil
Brand Names
Revatio, Viagra
FDA approval date: March 27, 1998
Classification: Phosphodiesterase 5 Inhibitor
Form: Injection, Tablet, Powder, For
What is Revatio (Sildenafil)?
Sildenafil tablets are indicated for the treatment of erectile dysfunction.
Approved To Treat
Top Global Experts
There are no experts for this drug
Save this treatment for later
Not sure about your diagnosis?
Related Clinical Trials
There is no clinical trials being done for this treatment
Related Latest Advances
There is no latest advances for this treatment
Brand Information
Revatio (sildenafil citrate)
1INDICATIONS AND USAGE
Adults
REVATIO is indicated for the treatment of pulmonary arterial hypertension (PAH) (World Health Organization [WHO] Group I) in adults to improve exercise ability and delay clinical worsening
Pediatric Patients (1 to 17 Years Old)
REVATIO is indicated in pediatric patients 1 to 17 years old for the treatment of pulmonary arterial hypertension (PAH) (WHO Group I) to improve exercise ability and, in pediatric patients too young to perform standardized exercise testing, pulmonary hemodynamics thought to underlie improvements in exercise
2DOSAGE FORMS AND STRENGTHS
REVATIO Tablets
White to off-white, film-coated, round tablets engraved with “RVT 20” on one side and “VLE” on the other side. Each tablet contains sildenafil citrate equivalent to 20 mg of sildenafil.
REVATIO for Oral Suspension
White to slight pink powder containing 1.57 g of sildenafil citrate (equivalent to 1.12 g sildenafil) in a bottle for reconstitution to 10 mg/mL. Following reconstitution with 90 mL of water, the total volume of the oral suspension is 112 mL. A 2 mL oral dosing syringe (with 1 mL and 2 mL dose markings) and a press-in bottle adaptor are also provided.
REVATIO Injection
Single-dose vial containing 10 mg/12.5 mL (0.8 mg/mL) of sildenafil.
3CONTRAINDICATIONS
REVATIO is contraindicated in patients with:
- Concomitant use of organic nitrates in any form, either regularly or intermittently, because of the greater risk of hypotension
- Concomitant use of riociguat, a guanylate cyclase stimulator. Phosphodiesterase-5 (PDE-5) inhibitors, including sildenafil, may potentiate the hypotensive effects of riociguat.
- Known hypersensitivity to sildenafil or any component of the tablet, injection, or oral suspension. Hypersensitivity, including anaphylactic reaction, anaphylactic shock and anaphylactoid reaction, has been reported in association with the use of sildenafil.
4ADVERSE REACTIONS
The following serious adverse events are discussed elsewhere in the labeling:
- Hypotension
- Vision Loss
- Hearing Loss
- Priapism
- Vaso-occlusive Crisis in Patients with Pulmonary Hypertension Secondary to Sickle Cell Disease
4.1Clinical Trials Experience
Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in practice.
In a 12-week, placebo-controlled clinical study and an open-label extension study (SUPER-1) in 277 REVATIO-treated adults with PAH (WHO Group I)
In a placebo-controlled fixed dose titration study (PACES-1) of REVATIO (starting with recommended dose of 20 mg and increased to 40 mg and then 80 mg all three times a day) as an adjunct to intravenous epoprostenol in patients with PAH, no new safety issues were identified except for edema, which occurred in 25% of subjects in the combined REVATIO + epoprostenol group compared with 13% of subjects in the epoprostenol group
In a study to assess the effects of multiple doses of REVATIO on mortality in adults with PAH (StudyA1481324), the lower dose 5 mg TID group showed a higher observed number of deaths (all related to underlying disease/disease under study), serious adverse events, and severe adverse events than the 20 mg and 80 mg TID groups
4.1.1Pediatric Patients
REVATIO was studied in a total of 234 PAH pediatric patients 1 to 17 years of age in a 16‑week, double-blind placebo‑controlled study (STARTS-1); 220 patients continued in a long-term extension study (STARTS-2). Erection increased was observed in 9% of patients treated with sildenafil in STARTS-1. No other new adverse reactions were identified in pediatric patients
4.1.2REVATIO Injection
Adverse events with REVATIO injection were similar to those seen with oral tablets.
4.2Postmarketing Experience
The following adverse reactions have been identified during post approval use of sildenafil (marketed for both PAH and erectile dysfunction). Because these reactions are reported voluntarily from a population of uncertain size, it is not always possible to reliably estimate their frequency or establish a causal relationship to drug exposure.
4.2.1Cardiovascular Events
In postmarketing experience with sildenafil at doses indicated for erectile dysfunction, serious cardiovascular, cerebrovascular, and vascular events, including myocardial infarction, sudden cardiac death, ventricular arrhythmia, cerebrovascular hemorrhage, transient ischemic attack, hypertension, pulmonary hemorrhage, and subarachnoid and intracerebral hemorrhages have been reported in temporal association with the use of the drug. Most, but not all, of these patients had preexisting cardiovascular risk factors. Many of these events were reported to occur during or shortly after sexual activity, and a few were reported to occur shortly after the use of sildenafil without sexual activity. Others were reported to have occurred hours to days after use concurrent with sexual activity. It is not possible to determine whether these events are related directly to sildenafil, to sexual activity, to the patient’s underlying cardiovascular disease, or to a combination of these or other factors.
4.2.2Nervous System
Seizure, seizure recurrence
4.2.3Ophthalmologic
NAION
5DRUG INTERACTIONS
Nitrates
Concomitant use of REVATIO with nitrates in any form is contraindicated
Strong CYP3A Inhibitors
Concomitant use of REVATIO with strong CYP3A inhibitors is not recommended
Moderate-to-Strong CYP3A Inducers
Concomitant use of REVATIO with moderate-to-strong CYP3A inducers (such as bosentan) decreases the sildenafil exposure. Dose up-titration of REVATIO may be needed when initiating treatment with moderate-to-strong CYP3A inducers. Reduce the dose of REVATIO to 20 mg three times a day when discontinuing treatment with moderate-to-strong CYP3A inducers
6OVERDOSAGE
In studies with healthy volunteers of single doses up to 800 mg, adverse events were similar to those seen at lower doses but rates and severities were increased.
In cases of overdose, standard supportive measures should be adopted as required. Renal dialysis is not expected to accelerate clearance as sildenafil is highly bound to plasma proteins and it is not eliminated in the urine.
7DESCRIPTION
REVATIO, phosphodiesterase-5 (PDE-5) inhibitor, is the citrate salt of sildenafil, a selective inhibitor of cyclic guanosine monophosphate (cGMP)-specific phosphodiesterase type-5 (PDE-5). Sildenafil is also marketed as VIAGRA
Sildenafil citrate is designated chemically as 1-[[3-(6,7-dihydro-1-methyl-7-oxo-3-propyl-1

Sildenafil citrate is a white to off-white crystalline powder with a solubility of 3.5 mg/mL in water and a molecular weight of 666.7.
REVATIO (sildenafil) Tablets: REVATIO is formulated as white to off-white, film-coated, round tablets for oral administration. Each tablet contains sildenafil citrate equivalent to 20 mg of sildenafil. In addition to the active ingredient, sildenafil citrate, each tablet contains the following inactive ingredients: anhydrous dibasic calcium phosphate, croscarmellose sodium, hypromellose, lactose monohydrate, magnesium stearate, microcrystalline cellulose, titanium dioxide, and triacetin.
REVATIO (sildenafil) Injection: REVATIO is supplied as a clear, colorless, sterile, ready to use solution in a single-dose vial containing 10 mg/12.5 mL of sildenafil. Each mL of solution contains 1.124 mg sildenafil citrate (equivalent to 0.8 mg sildenafil), 50.5 mg dextrose, and water for injection.
REVATIO (sildenafil) for Oral Suspension: REVATIO is supplied as white to slight pink powder containing 1.57 g of sildenafil citrate (equivalent to 1.12 g sildenafil) in an amber glass bottle intended for reconstitution. Following reconstitution with 90 mL water, the total volume of the oral suspension is 112 mL and the oral suspension contains 10 mg/mL sildenafil. The inactive ingredients include citric acid anhydrous, colloidal silicon dioxide anhydrous, grape flavor, sodium benzoate, sodium citrate dihydrate, sorbitol, sucralose, titanium dioxide, and xanthan gum. In addition to the bottle, a press-in bottle adapter and an oral dosing syringe (with 1 mL and 2 mL dose markings) are provided.
8CLINICAL STUDIES
SUPER-1 (NCT00644605) - REVATIO Monotherapy [20 mg, 40 mg, and 80 mg Three Times a Day]
A randomized, double-blind, placebo-controlled study of REVATIO (SUPER-1) was conducted in 277 patients with PAH (defined as a mean pulmonary artery pressure ≥ 25 mmHg at rest with a pulmonary capillary wedge pressure < 15 mmHg). Patients were predominantly WHO Functional Classes II-III. Allowed background therapy included a combination of anticoagulants, digoxin, calcium channel blockers, diuretics, and oxygen. The use of prostacyclin analogues, endothelin receptor antagonists, and arginine supplementation were not permitted. Patients who had failed to respond to bosentan were also excluded. Patients with left ventricular ejection fraction less than 45% or left ventricular shortening fraction less than 0.2 also were not studied.
Patients were randomized to receive placebo (n = 70) or REVATIO 20 mg (n = 69), 40 mg (n = 67) or 80 mg (n = 71) three times a day for a period of 12 weeks. They had either primary pulmonary hypertension (PPH) (63%), PAH associated with CTD (30%), or PAH following surgical repair of left-to-right congenital heart lesions (7%). The study population consisted of 25% men and 75% women with a mean age of 49 years (range: 18 to 81 years) and baseline 6-minute walk distance between 100 and 450 meters (mean 343).
The primary efficacy endpoint was the change from baseline at Week 12 (at least 4 hours after the last dose) in the 6-minute walk distance. Placebo-corrected mean increases in walk distance of 45-50 meters were observed with all doses of REVATIO. These increases were significantly different from placebo, but the REVATIO dose groups were not different from each other (see Figure 3), indicating no additional clinical benefit from doses higher than 20 mg three times a day. The improvement in walk distance was apparent after 4 weeks of treatment and was maintained at Week 8 and Week 12.

Figure 4 displays subgroup efficacy analyses in SUPER-1 for the change from baseline in 6-Minute Walk Distance at Week 12 including baseline walk distance, disease etiology, functional class, gender, age, and hemodynamic parameters.

Key: PAH = pulmonary arterial hypertension; CTD = connective tissue disease; PH = pulmonary hypertension; PAP = pulmonary arterial pressure; PVRI = pulmonary vascular resistance index; TID = three times daily.
SUPER-2 (NCT00159887) Long-Term Treatment of PAH
In a long-term follow-up of patients who were treated with sildenafil (n = 277), K-M estimates of survival at 1, 2, and 3 years were 94%, 88% , and 79%, respectively. These uncontrolled observations do not allow comparison with a group not given sildenafil and cannot be used to determine the long term-effect of sildenafil on mortality.
PACES-1 (NCT00159861) - REVATIO Co-Administered with Epoprostenol
A randomized, double-blind, placebo‑controlled study (PACES-1) was conducted in 267 patients with PAH who were taking stable doses of intravenous epoprostenol. Patients had to have a mean pulmonary artery pressure (mPAP) greater than or equal to 25 mmHg and a pulmonary capillary wedge pressure (PCWP) less than or equal to 15 mmHg at rest via right heart catheterization within 21 days before randomization, and a baseline 6-minute walk test distance greater than or equal to 100 meters and less than or equal to 450 meters (mean 349 meters). Patients were randomized to placebo or REVATIO (in a fixed titration starting from 20 mg to 40 mg and then 80 mg, three times a day) and all patients continued intravenous epoprostenol therapy.
At baseline patients had PPH (80%) or PAH secondary to CTD (20%); WHO Functional Class I (1%), II (26%), III (67%), or IV (6%); and the mean age was 48 years, 80% were female, and 79% were Caucasian.
There was a statistically significant greater increase from baseline in 6-minute walk distance at Week 16 (primary endpoint) for the REVATIO group compared with the placebo group. The mean change from baseline at Week 16 (last observation carried forward) was 30 meters for the REVATIO group compared with 4 meters for the placebo group giving an adjusted treatment difference of 26 meters (95% CI: 10.8, 41.2) (p = 0.0009).
Patients on REVATIO achieved a statistically significant reduction in mPAP compared to those on placebo. A mean placebo-corrected treatment effect of -3.9 mmHg was observed in favor of REVATIO (95% CI: -5.7, -2.1) (p = 0.00003).
Time to clinical worsening of PAH was defined as the time from randomization to the first occurrence of a clinical worsening event (death, lung transplantation, initiation of bosentan therapy, or clinical deterioration requiring a change in epoprostenol therapy). Table 4 displays the number of patients with clinical worsening events in PACES-1. Kaplan-Meier estimates and a stratified log-rank test demonstrated that placebo-treated patients were 3 times more likely to experience a clinical worsening event than REVATIO-treated patients and that REVATIO-treated patients experienced a significant delay in time to clinical worsening versus placebo-treated patients (p = 0.0074). Kaplan‑Meier plot of time to clinical worsening is presented in Figure 5.

Improvements in WHO Functional Class for PAH were also demonstrated in patients on REVATIO compared to placebo. More than twice as many REVATIO-treated patients (36%) as placebo-treated patients (14%) showed an improvement in at least one functional New York Heart Association (NYHA) class for PAH.
Study A1481243 (NCT00323297) - REVATIO Added to Bosentan Therapy – Lack of Effect on Exercise Capacity
A randomized, double-blind, placebo‑controlled study was conducted in 103 patients with PAH who were on bosentan therapy for a minimum of 3 months. The PAH patients included those with primary PAH and PAH associated with CTD. Patients were randomized to placebo or sildenafil (20 mg three times a day) in combination with bosentan (62.5 to 125 mg twice a day). The primary efficacy endpoint was the change from baseline at Week 12 in 6-minute walk distance (6MWD). The results indicate that there is no significant difference in mean change from baseline on 6MWD observed between sildenafil 20 mg plus bosentan and bosentan alone.
STARTS-1 (NCT00159913) - Sildenafil in Treatment-Naive Children, Aged 1 to 17 Years, with Pulmonary Arterial Hypertension
A total of 234 patients with PAH aged 1 to 17 years were treated in a randomized, double-blind, multi-center, placebo-controlled parallel group, dose-ranging study. Patients (38% male and 62% female) had body weight ≥ 8 kg and had idiopathic pulmonary arterial hypertension (33%), or PAH associated with congenital heart disease (systemic-to-pulmonary shunt 37%, surgical repair 30%). In this trial, 27% of patients were < 7 years old. Patients were WHO Functional Class I (32%), II (51%), III (15%), or IV (0.4%).
Patients were naïve for specific PAH therapy and the use of prostacyclin, prostacyclin analogues and endothelin receptor antagonists were not permitted in the study, and neither were arginine supplementation, nitrates, alpha-blockers and potent CYP450 3A4 inhibitors.
The primary objective of the study was to assess the effect of REVATIO on percent change from baseline in PVO
Patients were allocated to one of three sildenafil treatment groups (low, medium, or high) or placebo. Actual doses administered were dependent on body weight (see Table 5).
The proportion of patients receiving supportive medicinal products at baseline (anticoagulants, digoxin, calcium channel blockers, diuretics and/or oxygen) was similar in the combined sildenafil treatment group (48%) and the placebo treatment group (42%).
The primary endpoint was a percentage change in VO
A total of 45% of patients were evaluable for CPET, which comprised those children ≥ 7 years old and developmentally able to perform the test. Children < 7 years were evaluable only for the secondary endpoints.
Mean increases in VO

The estimated difference between the combined sildenafil doses and placebo was 8% (95% CI: -0.2 to 16). The results of the main analysis (combined dose groups versus placebo) were not statistically significant (p = 0.056).
The estimated difference between the sildenafil medium dose group and placebo was 11 ± 5% (95% CI: 2 to 21).
Impact on Hemodynamic Parameters
Dose related improvements were observed with PVRI and mPAP. Statistically significant PVRI reductions compared to placebo were seen with the sildenafil medium and high dose groups (18% [95% CI: -32% to -2%] and 27% [95% CI: -39% to -14%], respectively) but not the low dose group (2% (95% CI: -20%, 20%). The sildenafil medium and high dose groups displayed mPAP changes from baseline compared to placebo, of ‑3.5 mmHg (95% CI: ‑8.9, 1.9) and ‑7.3 mmHg (95% CI: ‑12.4, ‑2.1), respectively; while the low dose group showed little difference from placebo (difference of 1.6 mmHg [95% CI: -4.5, 7.6]). Improvements were observed with cardiac index with all three sildenafil groups over placebo, 10%, 4%, and 15% for the low, medium, and high dose groups, respectively
STARTS-2 (NCT00159874) - Long-Term Survival with Oral Sildenafil Monotherapy in Treatment-Naïve Pediatric Pulmonary Arterial Hypertension
Of the 234 pediatric patients treated in the short-term, placebo-controlled study, 220 patients entered the long-term extension study. Patients who had been in the placebo group in the short-term study were randomly reassigned to sildenafil treatment; patients weighing ≤ 20 kg entered the medium or high dose groups (1:2), while patients weighing > 20 kg entered the low, medium, or high dose groups (1:1:1). Of the total 229 patients who received sildenafil, there were 55, 74, and 100 patients in the low, medium, and high dose groups, respectively. Across the short-term and long-term studies, the overall duration of treatment from start of double-blind for individual patients ranged from 3 to 3,129 days. By sildenafil treatment group, median duration of sildenafil treatment was 1,696 days (excluding the 5 patients who received placebo in double-blind and were not treated in the long-term extension study).
Peak VO
Kaplan-Meier estimates of survival at 3 years in patients > 20 kg in weight at baseline were 94%, 93%, and 85% in the low, medium, and high dose groups, respectively; for patients ≤ 20 kg in weight at baseline, the survival estimates were 94% and 93% for patients in the medium and high dose groups, respectively
Study A1481324 (NCT02060487) - Study to Assess the Effects of REVATIO on Mortality in Adults with PAH
A study to assess the effects of multiple doses of sildenafil on mortality in adults with PAH was conducted following the observation of a higher risk of mortality in pediatric patients taking a high dose of REVATIO TID, based on body weight, compared to those taking a lower dose of REVATIO in the long-term extension of the pediatric clinical trial.
The study was a randomized, double-blind, parallel-group study in 385 adults with PAH. Patients were randomly assigned 1:1:1 to one of three treatment groups (5, 20, and 80 mg TID). Most patients were PAH treatment naïve (83%). For most patients the etiology of PAH was idiopathic (72%). The most common WHO Functional Class was Class III (58% of patients). Treatment groups were well balanced with respect to baseline demographics of strata history of PAH treatment and etiology of PAH, as well as the WHO Functional Class categories.
The primary objective of the study was to compare sildenafil 80 mg TID versus 5 mg TID for mortality, with success defined by ruling out twice the mortality at 80 mg.
The key secondary efficacy endpoint was time to first event of clinical worsening, defined as a composite endpoint of all-cause mortality, hospitalization for worsening PAH or disease progression. An additional secondary endpoint was 6MWD at Months 6 and 12.
Overall Survival
At the time of a planned interim analysis (50% deaths) it was identified that the primary efficacy objective of this protocol was met and therefore the study was stopped. Based on the primary efficacy endpoint (mortality), the non-inferiority of sildenafil 80 mg TID arm versus 5 mg TID arm was met using a 2-sided significance level of 0.003 for the interim analysis. Primary comparison of the 80 mg TID group to the 5 mg TID group yielded the HR (99.7% CI) = 0.51 (0.22, 1.21); i.e., non-inferiority was established.
Kaplan-Meier estimates of survival at 3 years were 66%, 79%, and 85% in the 5-, 20-, and 80-mg TID dose groups, respectively.
Clinical Worsening
Sildenafil 80 mg was also superior to 5 mg for time to first event of clinical worsening with HR (99.7% CI) = 0.44 (0.22, 0.89).
6MWD at Months 6 and 12
At baseline, the median of 6MWD for the intent‑to‑treat (ITT) population was 332 to 352 m. At Month 6, the median change from baseline was highest for sildenafil 80 mg TID with 28 m compared to 18 m and 19 m for sildenafil 5 mg TID and sildenafil 20 mg TID groups, respectively. The same was seen at Month 12, the median change from baseline for sildenafil 80 mg TID group was 33 m compared to 17 m for sildenafil 5 mg TID and 31 m in sildenafil 20 mg TID groups.
Overall, the safety data for sildenafil 20 mg TID and for the higher sildenafil 80 mg TID dose were consistent with the established safety profile of sildenafil in previous adult PAH studies
9HOW SUPPLIED/STORAGE AND HANDLING
REVATIO tablets are supplied as white to off-white, film-coated, round tablets containing sildenafil citrate equivalent to the nominally indicated amount of sildenafil as follows:
Recommended Storage for REVATIO Tablets: Store at controlled room temperature 20°C to 25°C (68°F to 77°F); excursions permitted to 15°C to 30°C (59°F to 86°F)
REVATIO injection is supplied as a clear, colorless, sterile, ready to use solution containing 10 mg sildenafil/12.5 mL (0.8 mg/mL) presented in a single-dose glass vial.
Recommended Storage for REVATIO Injection: Store at controlled room temperature 20°C to 25°C (68°F to 77°F); excursions permitted to 15°C to 30°C (59°F to 86°F)
REVATIO powder for oral suspension is supplied in amber glass bottles. Each bottle contains white to slight pink powder containing 1.57 g of sildenafil citrate (equivalent to 1.12 g sildenafil). Following reconstitution, the total volume of the oral suspension is 112 mL (10 mg sildenafil/mL). A 2 mL oral dosing syringe (with 1 mL and 2 mL dose markings) and a press-in bottle adaptor are also provided.
Recommended Storage for REVATIO for Oral Suspension: Store below 30°C (86°F) in the original package in order to protect from moisture.
Recommended Storage for Reconstituted Oral Suspension: Store below 30°C (86°F) or in refrigerator at 2°C to 8°C (36°F to 46°F). Do not freeze. The shelf-life of the reconstituted oral suspension is 60 days. Any remaining oral suspension should be discarded 60 days after reconstitution.
10PATIENT COUNSELING INFORMATION
Advise the patient to read the FDA-approved patient labeling (Patient Information and Instructions for Use).
- Inform patients of contraindication of REVATIO with regular and/or intermittent use of organic nitrates.
- Inform patients that sildenafil is also marketed as VIAGRA for erectile dysfunction. Advise patients taking REVATIO not to take VIAGRA or other PDE-5 inhibitors.
- Advise patients to seek immediate medical attention for a sudden loss of vision in one or both eyes while taking REVATIO. Such an event may be a sign of NAION.
- Advise patients to seek prompt medical attention in the event of sudden decrease or loss of hearing while taking REVATIO. These events may be accompanied by tinnitus and dizziness.
Distributed by:
© 2024 Viatris Inc.
REVATIO is a registered trademark of Viatris Specialty LLC, a Viatris Company.
UPJ:RVTTOSI:R2
11PATIENT INFORMATION
This Patient Information has been approved by the U.S. Food and Drug Administration. Revised: December 2024
12Instructions for Use
REVATIO (re-VAH-tee-oh)
(sildenafil)
oral suspension
(sildenafil)
oral suspension
Read this Instructions for Use before you start taking REVATIO oral suspension or giving REVATIO oral suspension to your child and each time you get a refill. There may be new information. This information does not take the place of talking to your healthcare provider about your or your child’s medical condition or treatment.
Important information:
- Ask your healthcare provider or pharmacist to show you how to measure and take or give your child’s prescribed dose of REVATIO oral suspension.
- Your pharmacist will mix (reconstitute) REVATIO oral suspension before it is given to you.
- Always use the oral dosing syringe that comes with REVATIO oral suspension. If your carton does not come with an oral dosing syringe, contact your pharmacist.
- Do not take or give REVATIO oral suspension if the bottle adaptor is not in the bottle. If the bottle adaptor is not in the bottle, contact your pharmacist.
- REVATIO oral suspension should not be mixed with any other medicine or flavoring.
Supplies you will need to take or give a dose of REVATIO oral suspension (See Figure A):
- 1 bottle of REVATIO oral suspension with pre-inserted bottle adaptor
- 1 oral dosing syringe (provided in the carton)

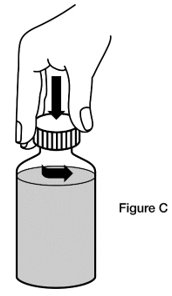
Step 1. Shake the bottle of REVATIO oral suspension for 10 seconds before each use. (See Figure B)

Step 2. Remove the cap. Open the bottle by pushing down on the cap and twisting it in the direction of the arrow (counter-clockwise). (See Figure C)
Step 3. Fully push down (depress) the plunger of the oral dosing syringe. Then insert the tip of the oral dosing syringe into the bottle adaptor while holding the bottle upright, on a flat surface. (See Figure D)

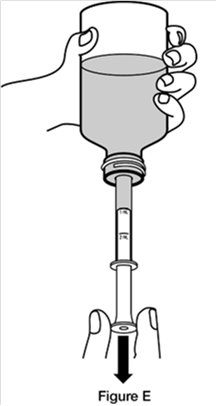
Step 4. Turn the bottle upside down while holding the oral dosing syringe in place. Slowly pull back the plunger of the oral dosing syringe until the bottom of the plunger is even with the mL marking on the syringe for your or your child’s prescribed dose. (See Figure E)
If you see air bubbles in the oral dosing syringe, slowly push the plunger all the way up so that REVATIO oral suspension flows back into the bottle and repeat Step 4.
Step 5. Turn the bottle back upright with the oral dosing syringe still in place. Place the bottle on a flat surface. Remove the oral dosing syringe from the bottle adaptor by pulling straight up on the barrel of the oral dosing syringe. (See Figure F)

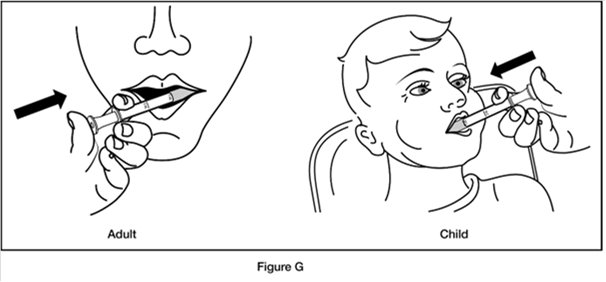
Step 6. Put the tip of the oral dosing syringe into your or your child’s mouth and point it towards the inside of the cheek. Slowly push the plunger of the oral dosing syringe all the way down to give the entire dose. Do not squirt the medicine out quickly. (See Figure G)
Step 7. Replace the cap on the bottle, leaving the bottle adaptor in place. Turn the cap in the direction of the arrow (clockwise) to close the bottle. (See Figure H)

Step 8. Wash the oral dosing syringe after each use. Pull the plunger out of the barrel and rinse both parts with water. (See Figure I)

Step 9. Dry all parts with a clean paper towel. Push the plunger back into the barrel. Store the oral dosing syringe with the REVATIO oral suspension bottle.
How should I store REVATIO?
- Store mixed (reconstituted) REVATIO oral suspension below 86°F (30°C) or in a refrigerator between 36°F to 46°F (2°C to 8°C).
- Do not freeze mixed REVATIO oral suspension.
- Throw away (discard) any remaining REVATIO oral suspension 60 days after mixed by the pharmacist. See the “Discard after” date written on the bottle label.
Keep REVATIO and all medicines out of the reach of children.
Distributed by:
© 2024 Viatris Inc.
REVATIO is a registered trademark of Viatris Specialty LLC, a Viatris Company.
UPJ:IFU:RVTTOSI:R2
This Instructions for Use has been approved by the U.S. Food and Drug Administration. Revised: December 2024
13PRINCIPAL DISPLAY PANEL – 20 mg
NDC 58151-402-77
Revatio
20 mg*
Rx only
90 Tablets
Store at controlled room
Dispense in tight containers
DOSAGE AND USE
See accompanying prescribing
information.
See accompanying prescribing
information.
*Each tablet contains sildenafil
Distributed by:
© 2024 Viatris Inc.
Made in France
RUPJ402MM
14PRINCIPAL DISPLAY PANEL – 10 mg/12.5 mL
NDC 58151-395-31
Sterile Single-dose
Rx only
Revatio
(sildenafil) Injection
(sildenafil) Injection
10 mg/12.5 mL
For Intravenous Use
Store at controlled room
[see USP Controlled Room
[see USP Controlled Room
Each mL of solution contains
DOSAGE AND USE
See accompanying prescribing
information.
See accompanying prescribing
information.
Distributed by:
© 2024 Viatris Inc.
REVATIO is a registered trademark
Made in France
UPJ:395:1C:R1

15PRINCIPAL DISPLAY PANEL – 10 mg/mL
NDC 58151-385-35
Rx only
Revatio®
10 mg/mL
For Oral Use Only
Shake Well Before Each Use
RECONSTITUTION DIRECTIONS:
112 mL following Reconstitution
Grape Flavored
Rx only
BEFORE RECONSTITUTION:
RECONSTITUTED SUSPENSION:
Each mL of the suspension contains 10 mg
Each bottle contains 1.57 g of sildenafil
RECOMMENDED DOSAGE: See prescribing
information.
An oral dosing syringe, and a press-in bottle
adaptor are also provided.
information.
An oral dosing syringe, and a press-in bottle
adaptor are also provided.
Distributed by:
© 2024 Viatris Inc.
REVATIO is a registered trademark of Viatris
Made in France
UPJ:385:1C:R1
