Brand Name
Zoloft
Generic Name
Sertraline
View Brand Information FDA approval date: February 11, 1992
Classification: Serotonin Reuptake Inhibitor
Form: Tablet, Capsule, Solution
What is Zoloft (Sertraline)?
Major Depressive Disorder– Sertraline hydrochloride tablets USP are indicated for the treatment of major depressive disorder in adults. The efficacy of sertraline hydrochloride in the treatment of a major depressive episode was established in six to eight week controlled trials of adult outpatients whose diagnoses corresponded most closely to the DSM-III category of major depressive disorder. A major depressive episode implies a prominent and relatively persistent depressed or dysphoric mood that usually interferes with daily functioning ; it should include at least 4 of the following 8 symptoms: change in appetite, change in sleep, psychomotor agitation or retardation, loss of interest in usual activities or decrease in sexual drive, increased fatigue, feelings of guilt or worthlessness, slowed thinking or impaired concentration, and a suicide attempt or suicidal ideation. The antidepressant action of sertraline hydrochloride in hospitalized depressed patients has not been adequately studied. The efficacy of sertraline hydrochloride in maintaining an antidepressant response for up to 44 weeks following 8 weeks of open-label acute treatment was demonstrated in a placebo-controlled trial. The usefulness of the drug in patients receiving sertraline hydrochloride for extended periods should be reevaluated periodically. Obsessive-Compulsive Disorder– Sertraline hydrochloride tablets USP are indicated for the treatment of obsessions and compulsions in patients with obsessive-compulsive disorder , as defined in the DSM-III-R; i.e., the obsessions or compulsions cause marked distress, are time-consuming, or significantly interfere with social or occupational functioning. The efficacy of sertraline hydrochloride was established in 12-week trials with obsessive-compulsive outpatients having diagnoses of obsessive-compulsive disorder as defined according to DSM-III or DSM-III-R criteria. Obsessive-compulsive disorder is characterized by recurrent and persistent ideas, thoughts, impulses, or images that are ego-dystonic and/or repetitive, purposeful, and intentional behaviors that are recognized by the person as excessive or unreasonable. The efficacy of sertraline hydrochloride in maintaining a response, in patients with OCD who responded during a 52-week treatment phase while taking sertraline hydrochloride and were then observed for relapse during a period of up to 28 weeks, was demonstrated in a placebo-controlled trial. Nevertheless, the physician who elects to use sertraline hydrochloride for extended periods should periodically re-evaluate the long-term usefulness of the drug for the individual patient. Panic Disorder– Sertraline hydrochloride tablets USP are indicated for the treatment of panic disorder in adults, with or without agoraphobia, as defined in DSM-IV. Panic disorder is characterized by the occurrence of unexpected panic attacks and associated concern about having additional attacks, worry about the implications or consequences of the attacks, and/or a significant change in behavior related to the attacks. The efficacy of sertraline hydrochloride was established in three 10 to 12 week trials in adult panic disorder patients whose diagnoses corresponded to the DSM-III-R category of panic disorder. Panic disorder is characterized by recurrent unexpected panic attacks, i.e., a discrete period of intense fear or discomfort in which four of the following symptoms develop abruptly and reach a peak within 10 minutes: palpitations, pounding heart, or accelerated heart rate; sweating; trembling or shaking; sensations of shortness of breath or smothering; feeling of choking; chest pain or discomfort; nausea or abdominal distress; feeling dizzy, unsteady, lightheaded, or faint; derealization or depersonalization ; fear of losing control; fear of dying; paresthesias ; chills or hot flushes. The efficacy of sertraline hydrochloride in maintaining a response, in adult patients with panic disorder who responded during a 52-week treatment phase while taking sertraline hydrochloride and were then observed for relapse during a period of up to 28 weeks, was demonstrated in a placebo-controlled trial. Nevertheless, the physician who elects to use sertraline hydrochloride for extended periods should periodically re-evaluate the long-term usefulness of the drug for the individual patient. Posttraumatic Stress Disorder – Sertraline hydrochloride tablets USP are indicated for the treatment of posttraumatic stress disorder in adults. The efficacy of sertraline hydrochloride in the treatment of PTSD was established in two 12-week placebo-controlled trials of adult outpatients whose diagnosis met criteria for the DSM-III-R category of PTSD. PTSD, as defined by DSM-III-R/IV, requires exposure to a traumatic event that involved actual or threatened death or serious injury, or threat to the physical integrity of self or others, and a response which involves intense fear, helplessness, or horror. Symptoms that occur as a result of exposure to the traumatic event include reexperiencing of the event in the form of intrusive thoughts, flashbacks or dreams, and intense psychological distress and physiological reactivity on exposure to cues to the event; avoidance of situations reminiscent of the traumatic event, inability to recall details of the event, and/or numbing of general responsiveness manifested as diminished interest in significant activities, estrangement from others, restricted range of affect, or sense of foreshortened future; and symptoms of autonomic arousal including hypervigilance, exaggerated startle response, sleep disturbance, impaired concentration, and irritability or outbursts of anger. A PTSD diagnosis requires that the symptoms are present for at least a month and that they cause clinically significant distress or impairment in social, occupational, or other important areas of functioning. The efficacy of sertraline hydrochloride in maintaining a response in adult patients with PTSD for up to 28 weeks following 24 weeks of open-label treatment was demonstrated in a placebo-controlled trial. Nevertheless, the physician who elects to use sertraline hydrochloride for extended periods should periodically re-evaluate the long-term usefulness of the drug for the individual patient. Premenstrual Dysphoric Disorder – Sertraline hydrochloride tablets USP are indicated for the treatment of premenstrual dysphoric disorder in adults. The efficacy of sertraline hydrochloride in the treatment of PMDD was established in 2 placebo-controlled trials of female adult outpatients treated for 3 menstrual cycles who met criteria for the DSM-III-R/IV category of PMDD. The essential features of PMDD include markedly depressed mood, anxiety or tension, affective lability, and persistent anger or irritability. Other features include decreased interest in activities, difficulty concentrating, lack of energy, change in appetite or sleep, and feeling out of control. Physical symptoms associated with PMDD include breast tenderness, headache, joint and muscle pain, bloating and weight gain. These symptoms occur regularly during the luteal phase and remit within a few days following onset of menses; the disturbance markedly interferes with work or school or with usual social activities and relationships with others. In making the diagnosis, care should be taken to rule out other cyclical mood disorders that may be exacerbated by treatment with an antidepressant. The effectiveness of sertraline hydrochloride in long-term use, that is, for more than 3 menstrual cycles, has not been systematically evaluated in controlled trials. Therefore, the physician who elects to use sertraline hydrochloride for extended periods should periodically re-evaluate the long-term usefulness of the drug for the individual patient. Social Anxiety Disorder– Sertraline hydrochloride tablets USP are indicated for the treatment of social anxiety disorder, also known as social phobia in adults. The efficacy of sertraline hydrochloride in the treatment of social anxiety disorder was established in two placebo-controlled trials of adult outpatients with a diagnosis of social anxiety disorder as defined by DSM-IV criteria. Social anxiety disorder, as defined by DSM-IV, is characterized by marked and persistent fear of social or performance situations involving exposure to unfamiliar people or possible scrutiny by others and by fears of acting in a humiliating or embarrassing way. Exposure to the feared social situation almost always provokes anxiety and feared social or performance situations are avoided or else are endured with intense anxiety or distress. In addition, patients recognize that the fear is excessive or unreasonable and the avoidance and anticipatory anxiety of the feared situation is associated with functional impairment or marked distress. The efficacy of sertraline hydrochloride in maintaining a response in adult patients with social anxiety disorder for up to 24 weeks following 20 weeks of sertraline hydrochloride treatment was demonstrated in a placebo-controlled trial. Physicians who prescribe sertraline hydrochloride tablets USP for extended periods should periodically re-evaluate the long-term usefulness of the drug for the individual patient.
Approved To Treat
Top Global Experts
There are no experts for this drug
Save this treatment for later
Not sure about your diagnosis?
Related Clinical Trials
There is no clinical trials being done for this treatment
Related Latest Advances
There is no latest advances for this treatment
Brand Information
Zoloft (sertraline hydrochloride)
WARNING: SUICIDAL THOUGHTS AND BEHAVIORS
Antidepressants increased the risk of suicidal thoughts and behavior in pediatric and young adult patients in short-term studies. Closely monitor all antidepressant-treated patients for clinical worsening, and for emergence of suicidal thoughts and behaviors
1INDICATIONS AND USAGE
ZOLOFT is indicated for the treatment of the following
- Major depressive disorder (MDD)
- Obsessive-compulsive disorder (OCD)
- Panic disorder (PD)
- Posttraumatic stress disorder (PTSD)
- Social anxiety disorder (SAD)
- Premenstrual dysphoric disorder (PMDD)
2DOSAGE FORMS AND STRENGTHS
25 mg tablets: light green film-coated, engraved on one side with “ZOLOFT” and on the other side scored and engraved with “25 mg”
50 mg tablets: light blue film-coated, engraved on one side with “ZOLOFT” and on the other side scored and engraved with “50 mg”
100 mg tablets: light yellow film-coated, engraved on one side with “ZOLOFT” and on the other side scored and engraved with “100 mg”
Oral solution: a clear, colorless solution with a menthol scent containing sertraline hydrochloride equivalent to 20 mg of sertraline per mL and 12% alcohol. It is supplied as a 60 mL bottle with an accompanying calibrated dropper that has 25 mg and 50 mg graduation marks.
3CONTRAINDICATIONS
ZOLOFT is contraindicated in patients:
- Taking, or within 14 days of stopping, MAOIs, (including the MAOIs linezolid and intravenous methylene blue) because of an increased risk of serotonin syndrome
- Taking pimozide
- With known hypersensitivity to sertraline (e.g., anaphylaxis, angioedema)
In addition to the contraindications for all ZOLOFT formulations listed above, ZOLOFT oral solution is contraindicated in patients:
- Taking disulfiram. ZOLOFT oral solution contains alcohol, and concomitant use of ZOLOFT and disulfiram may result in a disulfiram-alcohol reaction.
4ADVERSE REACTIONS
The following adverse reactions are described in more detail in other sections of the prescribing information:
- Hypersensitivity reactions to sertraline
- Disulfiram-alcohol reaction when ZOLOFT oral solution is taken with disulfiram
- QTc prolongation and ventricular arrhythmias when taken with pimozide
- Suicidal thoughts and behaviors
- Serotonin syndrome
- Increased risk of bleeding
- Activation of mania/hypomania
- Discontinuation syndrome
- Seizures
- Angle-closure glaucoma
- Hyponatremia
- Sexual Dysfunction
4.1Clinical Trials Experience
Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in practice.
The data described below are from randomized, double-blind, placebo-controlled trials of ZOLOFT (mostly 50 mg to 200 mg per day) in 3066 adults diagnosed with MDD, OCD, PD, PTSD, SAD, and PMDD. These 3066 patients exposed to ZOLOFT for 8 to12 weeks represent 568 patient-years of exposure. The mean age was 40 years; 57% were females and 43% were males.
The most common adverse reactions (≥5% and twice placebo) in all pooled placebo-controlled clinical trials of all ZOLOFT-treated patients with MDD, OCD, PD, PTSD, SAD and PMDD were nausea, diarrhea/loose stool, tremor, dyspepsia, decreased appetite, hyperhidrosis, ejaculation failure, and decreased libido (see Table 3). The following are the most common adverse reactions in trials of ZOLOFT (≥5% and twice placebo) by indication that were not mentioned previously.
- MDD: somnolence;
- OCD: insomnia, agitation;
- PD: constipation, agitation;
- PTSD: fatigue;
- PMDD: somnolence, dry mouth, dizziness, fatigue, and abdominal pain;
- SAD: insomnia, dizziness, fatigue, dry mouth, malaise.
Adverse Reactions Leading to Discontinuation in Placebo-Controlled Clinical Trials
In all placebo-controlled studies in patients with MDD, OCD, PD, PTSD, SAD and PMDD, 368 (12%) of the 3066 patients who received ZOLOFT discontinued treatment due to an adverse reaction, compared with 93 (4%) of the 2293 placebo-treated patients. In placebo-controlled studies, the following were the common adverse reactions leading to discontinuation in ZOLOFT-treated patients:
- MDD, OCD, PD, PTSD, SAD and PMDD: nausea (3%), diarrhea (2%), agitation (2%), and insomnia (2%).
- MDD (>2% and twice placebo): decreased appetite, dizziness, fatigue, headache, somnolence, tremor, and vomiting.
- OCD: somnolence.
- PD: nervousness and somnolence.
Male and Female Sexual Dysfunction
Although changes in sexual desire, sexual performance and sexual satisfaction often occur as manifestations of a psychiatric disorder, they may also be a consequence of SSRI treatment. However, reliable estimates of the incidence and severity of untoward experiences involving sexual desire, performance and satisfaction are difficult to obtain, in part because patients and healthcare providers may be reluctant to discuss them. Accordingly, estimates of the incidence of untoward sexual experience and performance cited in labeling may underestimate their actual incidence.
Table 4 below displays the incidence of sexual adverse reactions reported by at least 2% of ZOLOFT-treated patients and twice placebo from pooled placebo-controlled trials. For men and all indications, the most common adverse reactions (>2% and twice placebo) included: ejaculation failure, decreased libido, erectile dysfunction, ejaculation disorder, and male sexual dysfunction. For women, the most common adverse reaction (≥2% and twice placebo) was decreased libido.
Adverse Reactions in Pediatric Patients
In 281 pediatric patients treated with ZOLOFT in placebo-controlled studies, the overall profile of adverse reactions was generally similar to that seen in adult studies. Adverse reactions that do not appear in Table 3 (most common adverse reactions in adults) yet were reported in at least 2% of pediatric patients and at a rate of at least twice the placebo rate include fever, hyperkinesia, urinary incontinence, aggression, epistaxis, purpura, arthralgia, decreased weight, muscle twitching, and anxiety.
Other Adverse Reactions Observed During the Premarketing Evaluation of ZOLOFT
Other infrequent adverse reactions, not described elsewhere in the prescribing information, occurring at an incidence of < 2% in patients treated with ZOLOFT were:
Cardiac disorders - tachycardia
Ear and labyrinth disorders - tinnitus
Endocrine disorders - hypothyroidism
Eye disorders - mydriasis, blurred vision
Gastrointestinal disorders - hematochezia, melena, rectal hemorrhage
General disorders and administration site conditions - edema, gait disturbance, irritability, pyrexia
Hepatobiliary disorders - elevated liver enzymes
Immune system disorders - anaphylaxis
Metabolism and nutrition disorders - diabetes mellitus, hypercholesterolemia, hypoglycemia, increased appetite
Musculoskeletal and connective tissue disorders - arthralgia, muscle spasms, tightness, or twitching
Nervous system disorders - ataxia, coma, convulsion, decreased alertness, hypoesthesia, lethargy, psychomotor hyperactivity, syncope
Psychiatric disorders - aggression, bruxism, confusional state, euphoric mood, hallucination
Renal and urinary disorders - hematuria
Reproductive system and breast disorders - galactorrhea, priapism, vaginal hemorrhage
Respiratory, thoracic and mediastinal disorders - bronchospasm, epistaxis, yawning
Skin and subcutaneous tissue disorders - alopecia; cold sweat; dermatitis; dermatitis bullous; pruritus; purpura; erythematous, follicular, or maculopapular rash; urticaria
Vascular disorders - hemorrhage, hypertension, vasodilation
4.2Post-marketing Experience
The following adverse reactions have been identified during postapproval use of ZOLOFT. Because these reactions are reported voluntarily from a population of uncertain size, it is not always possible to reliably estimate their frequency or establish a causal relationship to drug exposure.
Bleeding or clotting disorders - increased coagulation times (altered platelet function)
Cardiac disorders - AV block, bradycardia, atrial arrhythmias, QTc-interval prolongation, ventricular tachycardia (including Torsade de Pointes) [See
Endocrine disorders - gynecomastia, hyperprolactinemia, menstrual irregularities, SIADH
Eye disorders - blindness, optic neuritis, cataract
Hepatobiliary disorders - severe liver events (including hepatitis, jaundice, liver failure with some fatal outcomes), pancreatitis
Hemic and lymphatic disorders - agranulocytosis, aplastic anemia and pancytopenia, leukopenia, thrombocytopenia, lupus-like syndrome, serum sickness
Immune system disorders - angioedema
Metabolism and nutrition disorders - hyponatremia, hyperglycemia
Musculoskeletal and connective tissue disorders - rhabdomyolysis, trismus
Nervous system disorders - serotonin syndrome, extrapyramidal symptoms (including akathisia and dystonia), oculogyric crisis
Psychiatric disorders - psychosis, enuresis, paroniria
Renal and urinary disorders - acute renal failure
Respiratory, thoracic and mediastinal disorders - pulmonary hypertension, eosinophilic pneumonia, anosmia, hyposmia
Skin and subcutaneous tissue disorders - photosensitivity skin reaction and other severe cutaneous reactions, which potentially can be fatal, such as Stevens-Johnson Syndrome (SJS) and toxic epidermal necrolysis (TEN)
Vascular disorders - cerebrovascular spasm (including reversible cerebral vasoconstriction syndrome and Call‑Fleming syndrome), vasculitis
5OVERDOSAGE
The following have been reported with sertraline tablet overdosage:
- Seizures, which may be delayed, and altered mental status including coma.
- Cardiovascular toxicity, which may be delayed, including QRS and QTc interval prolongation. Hypertension most commonly seen, but rarely can see hypotension alone or with co-ingestants including alcohol.
- Serotonin syndrome (patients with a multiple drug overdosage with other proserotonergic drugs may have a higher risk).
Gastrointestinal decontamination with activated charcoal should be considered in patients who present early after a sertraline overdose. Consider contacting a Poison Center (1-800-221-2222) or a medical toxicologist for additional overdosage management recommendations.
6DESCRIPTION
ZOLOFT contains sertraline hydrochloride, an SSRI. Sertraline hydrochloride has a molecular weight of 342.7 and has the following chemical name: (1S‑cis)‑4‑(3,4‑dichlorophenyl)‑1,2,3,4‑tetrahydro-N‑methyl‑1‑naphthalenamine hydrochloride. The empirical formula C
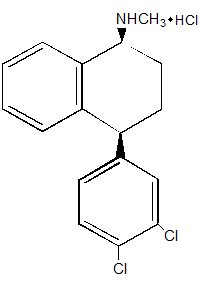
Sertraline hydrochloride is a white crystalline powder that is slightly soluble in water and isopropyl alcohol, and sparingly soluble in ethanol.
ZOLOFT tablets for oral administration contain 28.0 mg, 56.0 mg and 111.9 mg sertraline hydrochloride equivalent to 25, 50 and 100 mg of sertraline and the following inactive ingredients: dibasic calcium phosphate dihydrate, D & C Yellow #10 aluminum lake (in 25 mg tablet), FD & C Blue #1 aluminum lake (in 25 mg tablet), FD & C Red #40 aluminum lake (in 25 mg tablet), FD & C Blue #2 aluminum lake (in 50 mg tablet), hydroxypropyl cellulose, hypromellose, magnesium stearate, microcrystalline cellulose, polyethylene glycol, polysorbate 80, sodium starch glycolate, synthetic yellow iron oxide (in 100 mg tablet), and titanium dioxide.
ZOLOFT oral solution is available in a multidose 60 mL bottle. Each mL of solution contains 22.4 mg sertraline hydrochloride equivalent to 20 mg of sertraline. The solution contains the following inactive ingredients: glycerin, alcohol (12%), menthol, butylated hydroxytoluene (BHT). The oral solution must be diluted prior to administration
7CLINICAL STUDIES
Efficacy of ZOLOFT was established in the following trials:
- MDD: two short-term trials and one maintenance trials in adults
- OCD: three short-term trials in adults and one short-term trial in pediatric patients
- PD: three short-term trials and one maintenance trial in adults
- PTSD: two short-term trials and one maintenance trial in adults
- SAD: two short-term trials and one maintenance trial in adults
- PMDD: two short-term trials in adult female patients
7.1Major Depressive Disorder
The efficacy of ZOLOFT as a treatment for MDD was established in two randomized, double-blind, placebo-controlled studies and one double-blind, randomized-withdrawal study following an open label study in adult (ages 18 to 65) outpatients who met the Diagnostic and Statistical Manual of Mental Disorders (DSM-III) criteria for MDD (studies MDD-1 and MDD-2).
- Study MDD-1 was an 8-week, 3-arm study with flexible dosing of ZOLOFT, amitriptyline, and placebo. Adult patients received ZOLOFT (N=126, in a daily dose titrated weekly to 50 mg, 100 mg, or 200 mg), amitriptyline (N=123, in a daily dose titrated weekly to 50 mg, 100 mg, or 150 mg), or placebo (N= 130).
- Study MDD-2 was a 6-week, multicenter parallel study of three fixed doses of ZOLOFT administered once daily at 50 mg (N=82), 100 mg (N=75), and 200 mg (N=56) doses and placebo (N=76) in the treatment of adult outpatients with MDD.
Overall, these studies demonstrated ZOLOFT to be superior to placebo on the Hamilton Rating Scale for Depression (HAMD-17) and the Clinical Global Impression Severity (CGI-S) of Illness and Global Improvement (CGI-I) scores. Study MDD-2 was not readily interpretable regarding a dose response relationship for effectiveness.
A third study (Study MDD-3) involved adult outpatients meeting the DSM-III criteria for MDD who had responded by the end of an initial 8-week open treatment phase on ZOLOFT 50-200 mg/day. These patients (n=295) were randomized to continuation on double-blind ZOLOFT 50-200 mg/day or placebo for 44 weeks. A statistically significantly lower relapse rate was observed for patients taking ZOLOFT compared to those on placebo: ZOLOFT [n=11 (8%)] and placebo [n=31 (39%)]. The mean ZOLOFT dose for completers was 70 mg/day.
Analyses for gender effects on outcome did not suggest any differential responsiveness on the basis of sex.
7.2Panic Disorder
The effectiveness of ZOLOFT in the treatment of PD was demonstrated in three double‑blind, placebo‑controlled studies (Studies PD-1, PD-2, and PD‑3) of adult outpatients who had a primary diagnosis of PD (DSM‑III‑R), with or without agoraphobia.
- Studies PD-1 and PD-2 were 10-week flexible dose studies of ZOLOFT (N=80 study PD-1 and N=88 study PD-2) compared to placebo (N=176 study PD-1 and PD-2). In both studies, ZOLOFT was initiated at 25 mg/day for the first week, then titrated in weekly increments of 50 mg per day to a maximum dose of 200 mg/day on the basis of clinical response and toleration. The mean ZOLOFT doses for completers to 10 weeks were 131 mg/day and 144 mg/day, respectively, for Studies PD-1 and PD-2. In these studies, ZOLOFT was shown to be statistically significantly more effective than placebo on change from baseline in panic attack frequency and on the Clinical Global Impression Severity (CGI-S) of Illness and Global Improvement (CGI-I) scores. The difference between ZOLOFT and placebo in reduction from baseline in the number of full panic attacks was approximately 2 panic attacks per week in both studies.
- Study PD-3 was a 12-week randomized, double-blind fixed-dose study, including ZOLOFT doses of 50, 100, and 200 mg/day. Patients receiving ZOLOFT (50 mg N=43, 100 mg N=44, 200 mg N=45) experienced a statistically significantly greater reduction in panic attack frequency than patients receiving placebo (N=45). Study PD-3 was not readily interpretable regarding a dose response relationship for effectiveness.
Subgroup analyses did not indicate that there were any differences in treatment outcomes as a function of age, race, or gender.
In Study PD-4, patients meeting DSM-III-R criteria for PD who had responded during a 52-week open trial on ZOLOFT 50-200 mg/day (n=183) were randomized to continuation of ZOLOFT or to substitution of placebo for up to 28 weeks of observation for discontinuation due to relapse or insufficient clinical response. Response during the open phase was defined as a CGI-I score of 1(very much improved) or 2 (much improved). Insufficient clinical response in the double-blind phase indicated a worsening of the patient’s condition that resulted in study discontinuation, as assessed by the investigator. Relapse during the double-blind phase was defined as the following conditions being met on three consecutive visits:
(1) CGI-I ≥ 3;
(2) meets DSM-III-R criteria for PD;
(3) number of panic attacks greater than at baseline.
Patients receiving continued ZOLOFT treatment experienced a statistically significantly lower rate of discontinuation due to relapse or insufficient clinical response over the subsequent 28 weeks compared to those receiving placebo. This pattern was demonstrated in male and female subjects.
7.3Posttraumatic Stress Disorder
The effectiveness of ZOLOFT in the treatment of PTSD was established in two multicenter placebo‑controlled studies (Studies PSTD-1 and PSTD-2) of adult outpatients who met DSM‑III‑R criteria for PTSD. The mean duration of PTSD for these patients was 12 years (Studies PSTD-1 and PSTD-2 combined) and 44% of patients (169 of the 385 patients treated) had secondary depressive disorder.
Studies PSTD-1 and PSTD-2 were 12‑week flexible dose studies. ZOLOFT was initiated at 25 mg/day for the first week, and titrated in weekly increments of 50 mg per day to a maximum dose of 200 mg/day on the basis of clinical response and tolerability. The mean ZOLOFT dose for completers was 146 mg/day and 151 mg/day, respectively, for Studies PSTD-1 and PSTD-2. Study outcome was assessed by the Clinician‑Administered PTSD Scale Part 2 (CAPS), which is a multi‑item instrument that measures the three PTSD diagnostic symptom clusters of reexperiencing/intrusion, avoidance/numbing, and hyperarousal as well as the patient‑rated Impact of Event Scale (IES), which measures intrusion and avoidance symptoms. Patients receiving ZOLOFT (N=99 and N=94, respectively) showed statistically significant improvement compared to placebo (N=83 and N=92) on change from baseline to endpoint on the CAPS, IES, and on the Clinical Global Impressions (CGI-S) Severity of Illness and Global Improvement (CGI-I) scores.
In two additional placebo-controlled PTSD trials (Studies PSTD-3 and PSTD-4), the difference in response to treatment between patients receiving ZOLOFT and patients receiving placebo was not statistically significant. One of these additional studies was conducted in patients similar to those recruited for Studies PSTD-1 and PSTD-2, while the second additional study was conducted in predominantly male veterans.
As PTSD is a more common disorder in women than men, the majority (76%) of patients in Studies PSTD-1 and PSTD-2 described above were women. Post hoc exploratory analyses revealed a statistically significant difference between ZOLOFT and placebo on the CAPS, IES and CGI in women, regardless of baseline diagnosis of comorbid major depressive disorder, but essentially no effect in the relatively smaller number of men in these studies. The clinical significance of this apparent gender effect is unknown at this time. There was insufficient information to determine the effect of race or age on outcome.
In Study PSTD-5, patients meeting DSM-III-R criteria for PTSD who had responded during a 24-week open trial on ZOLOFT 50-200 mg/day (n=96) were randomized to continuation of ZOLOFT or to substitution of placebo for up to 28 weeks of observation for relapse. Response during the open phase was defined as a CGI-I of 1 (very much improved) or 2 (much improved), and a decrease in the CAPS-2 score of > 30% compared to baseline. Relapse during the double-blind phase was defined as the following conditions being met on two consecutive visits:
(1) CGI-I ≥ 3;
(2) CAPS-2 score increased by ≥ 30% and by ≥ 15 points relative to baseline; and
(3) worsening of the patient's condition in the investigator's judgment.
Patients receiving continued ZOLOFT treatment experienced statistically significantly lower relapse rates over the subsequent 28 weeks compared to those receiving placebo. This pattern was demonstrated in male and female subjects.
7.4Social Anxiety Disorder
The effectiveness of ZOLOFT in the treatment of SAD (also known as social phobia) was established in two multicenter, randomized, placebo-controlled studies (Study SAD-1 and SAD-2) of adult outpatients who met DSM-IV criteria for SAD.
Study SAD-1 was a 12-week, flexible dose study comparing ZOLOFT (50-200 mg/day), n=211, to placebo, n=204, in which ZOLOFT was initiated at 25 mg/day for the first week, then titrated to the maximum tolerated dose in 50 mg increments biweekly. Study outcomes were assessed by the:
(1) Liebowitz Social Anxiety Scale (LSAS), a 24-item clinician administered instrument that measures fear, anxiety, and avoidance of social and performance situations, and
(2) Proportion of responders as defined by the Clinical Global Impression of Improvement (CGI-I) criterion of CGI-I ≤ 2 (very much or much improved).
ZOLOFT was statistically significantly more effective than placebo as measured by the LSAS and the percentage of responders.
Study SAD-2 was a 20-week, flexible dose study that compared ZOLOFT (50-200 mg/day), n=135, to placebo, n=69. ZOLOFT was titrated to the maximum tolerated dose in 50 mg increments every 3 weeks. Study outcome was assessed by the:
(1) Duke Brief Social Phobia Scale (BSPS), a multi-item clinician-rated instrument that measures fear, avoidance and physiologic response to social or performance situations,
(2) Marks Fear Questionnaire Social Phobia Subscale (FQ-SPS), a 5-item patient-rated instrument that measures change in the severity of phobic avoidance and distress, and
(3) CGI-I responder criterion of ≤ 2.
ZOLOFT was shown to be statistically significantly more effective than placebo as measured by the BSPS total score and fear, avoidance and physiologic factor scores, as well as the FQ-SPS total score, and to have statistically significantly more responders than placebo as defined by the CGI-I. Subgroup analyses did not suggest differences in treatment outcome on the basis of gender. There was insufficient information to determine the effect of race or age on outcome.
In Study SAD-3, patients meeting DSM-IV criteria for SAD who had responded while assigned to ZOLOFT (CGI-I of 1 or 2) during a 20-week placebo-controlled trial on ZOLOFT 50-200 mg/day were randomized to continuation of ZOLOFT or to substitution of placebo for up to 24 weeks of observation for relapse. Relapse was defined as ≥ 2 point increase in the Clinical Global Impression Severity of Illness (CGI-S) score compared to baseline or study discontinuation due to lack of efficacy. Patients receiving ZOLOFT continuation treatment experienced a statistically significantly lower relapse rate during this 24-week period than patients randomized to placebo substitution.
7.5Premenstrual Dysphoric Disorder
The effectiveness of ZOLOFT for the treatment of PMDD was established in two double-blind, parallel group, placebo-controlled flexible dose trials (Studies PMDD-1 and PMDD-2) conducted over 3 menstrual cycles in adult female patients. The effectiveness of ZOLOFT for PMDD for more than 3 menstrual cycles has not been systematically evaluated in controlled trials.
Patients in Study PMDD-1 met DSM-III-R criteria for Late Luteal Phase Dysphoric Disorder (LLPDD), the clinical entity referred to as PMDD in DSM-IV. Patients in Study PMDD-2 met DSM-IV criteria for PMDD. Study PMDD-1 utilized continuous daily dosing throughout the study, while Study PMDD-2 utilized luteal phase dosing (intermittent dosing) for the 2 weeks prior to the onset of menses. The mean duration of PMDD symptoms was approximately 10.5 years in both studies. Patients taking oral contraceptives were excluded from these trials; therefore, the efficacy of ZOLOFT in combination with oral contraceptives for the treatment of PMDD is unknown.
Efficacy was assessed with the Daily Record of Severity of Problems (DRSP), a patient-rated instrument that mirrors the diagnostic criteria for PMDD as identified in the DSM-IV, and includes assessments for mood, physical symptoms, and other symptoms. Other efficacy assessments included the Hamilton Rating Scale for Depression (HAMD-17), and the Clinical Global Impression Severity of Illness (CGI-S) and Improvement (CGI-I) scores.
- In Study PMDD-1, involving 251 randomized patients, (n=125 on ZOLOFT and n=126 on placebo), ZOLOFT treatment was initiated at 50 mg/day and administered daily throughout the menstrual cycle. In subsequent cycles, ZOLOFT was titrated in 50 mg increments at the beginning of each menstrual cycle up to a maximum of 150 mg/day on the basis of clinical response and tolerability. The mean dose for completers was 102 mg/day. ZOLOFT administered daily throughout the menstrual cycle was statistically significantly more effective than placebo on change from baseline to endpoint on the DRSP total score, the HAMD-17 total score, and the CGI-S score, as well as the CGI-I score at endpoint.
- In Study PMDD-2, involving 281 randomized patients, (n=142 on ZOLOFT and n=139 on placebo), ZOLOFT treatment was initiated at 50 mg/day in the late luteal phase (last 2 weeks) of each menstrual cycle and then discontinued at the onset of menses (intermittent dosing). In subsequent cycles, patients were dosed in the range of 50-100 mg/day in the luteal phase of each cycle, on the basis of clinical response and tolerability. Patients who received 100 mg/day started with 50 mg/day for the first 3 days of the cycle, then 100 mg/day for the remainder of the cycle. The mean ZOLOFT dose for completers was 74 mg/day. ZOLOFT administered in the late luteal phase of the menstrual cycle was statistically significantly more effective than placebo on change from baseline to endpoint on the DRSP total score and the CGI-S score, as well as the CGI-I score at endpoint (Week 12).
There was insufficient information to determine the effect of race or age on outcome in these studies.
8HOW SUPPLIED/STORAGE AND HANDLING
ZOLOFT 25 mg tablets: light green, film-coated, capsular-shaped tablets engraved on one side with “ZOLOFT” and on the other side scored and engraved with “25 mg”
NDC 58151-574-93 Bottles of 30
ZOLOFT 50 mg tablets: light blue, film-coated, capsular-shaped tablets engraved on one side with “ZOLOFT” and on the other side scored and engraved with “50 mg”
NDC 58151-575-93 Bottles of 30
NDC 58151-575-88 Unit Dose Packages of 100
ZOLOFT 100 mg tablets: light yellow, film-coated, capsular-shaped, tablets engraved on one side with “ZOLOFT” and on the other side scored and engraved with “100 mg”
NDC 58151-576-93 Bottles of 30
NDC 58151-576-88 Unit Dose Packages of 100
ZOLOFT oral solution: clear, colorless solution with a menthol scent containing sertraline hydrochloride equivalent to 20 mg of sertraline per mL and 12% alcohol
NDC 58151-601-35 Bottles containing 60 mL, each with an accompanying calibrated dropper that has 25 mg and 50 mg graduation marks.
Store ZOLOFT at 20°C to 25°C (68°F to 77°F); excursions permitted to 15°C to 30°C (59°F to 86°F) [See USP Controlled Room Temperature].
9PATIENT COUNSELING INFORMATION
Advise the patient to read the FDA-approved patient labeling (Medication Guide).
Suicidal Thoughts and Behaviors
Advise patients and caregivers to look for the emergence of suicidality, especially early during treatment and when the dosage is adjusted up or down, and instruct them to report such symptoms to the healthcare provider
Important Administration Instructions for Oral Solution
For patients prescribed ZOLOFT oral solution, inform them that:
- ZOLOFT oral solution must be diluted before use. Do not mix in advance.
- Use the dropper provided to remove the required amount of ZOLOFT oral solution and mix with 4 ounces (1/2 cup) of water, ginger ale, lemon/lime soda, lemonade or orange juice ONLY. Do not mix ZOLOFT oral solution with anything other than the liquids listed.
- Take the dose immediately after mixing. At times, a slight haze may appear after mixing; this is normal.
- The dropper dispenser contains dry natural rubber, a consideration for patients with latex sensitivity.
Disulfiram Contraindication for ZOLOFT Oral Solution
Inform patients not to take disulfiram when taking ZOLOFT oral solution. Concomitant use is contraindicated due the alcohol content of the oral solution
Serotonin Syndrome
Caution patients about the risk of serotonin syndrome, particularly with the concomitant use of ZOLOFT with other serotonergic drugs including triptans, tricyclic antidepressants, opioids, lithium, tryptophan, buspirone, amphetamines, St. John’s Wort, and with drugs that impair metabolism of serotonin (in particular, MAOIs, both those intended to treat psychiatric disorders and also others, such as linezolid). Patients should contact their health care provider or report to the emergency room if they experience signs or symptoms of serotonin syndrome
Increased Risk of Bleeding
Inform patients about the concomitant use of ZOLOFT with aspirin, NSAIDs, other antiplatelet drugs, warfarin, or other anticoagulants because the combined use has been associated with an increased risk of bleeding. Advise patients to inform their health care providers if they are taking or planning to take any prescription or over-the-counter medications that increase the risk of bleeding
Activation of Mania/Hypomania
Advise patients and their caregivers to observe for signs of activation of mania/hypomania and instruct them to report such symptoms to the healthcare provider
Discontinuation Syndrome
Advise patients not to abruptly discontinue ZOLOFT and to discuss any tapering regimen with their healthcare provider. Adverse reactions can occur when ZOLOFT is discontinued
Sexual Dysfunction
Advise patients that use of ZOLOFT may cause symptoms of sexual dysfunction in both male and female patients. Inform patients that they should discuss any changes in sexual function and potential management strategies with their healthcare provider
Allergic Reactions
Advise patients to notify their healthcare provider if they develop an allergic reaction such as rash, hives, swelling, or difficulty breathing
Pregnancy
Inform pregnant women that ZOLOFT may cause withdrawal symptoms in the newborn or persistent pulmonary hypertension of the newborn (PPHN)
Distributed by:
© 2023 Viatris Inc.
ZOLOFT is a registered trademark of Viatris Specialty LLC a Viatris Company.
The brands listed are trademarks of their respective owners.
UPJ:ZLFTTOS:R1
10Medication Guide
This Medication Guide has been approved by the U.S. Food and Drug Administration. Revised: 8/2023
11PRINCIPAL DISPLAY PANEL – 25 mg
ALWAYS DISPENSE WITH MEDICATION GUIDE
NDC 58151-574-93
Zoloft
30 Tablets Rx only
Store at 20°C to 25°C (68°F to
DOSAGE AND USESee accompanying
prescribing information.
prescribing information.
*Each tablet contains 28.0 mg
Distributed by:
© 2023 Viatris Inc.
Made in Germany
RUPJ574H
12PRINCIPAL DISPLAY PANEL – 50 mg
ALWAYS DISPENSE WITH MEDICATION GUIDE
NDC 58151-575-93
Zoloft
30 Tablets Rx only
Store at 20°C to 25°C (68°F to
DOSAGE AND USESee accompanying
prescribing information.
prescribing information.
*Each tablet contains 56.0 mg
Distributed by:
© 2023 Viatris Inc.
Made in Germany
RUPJ575H
13PRINCIPAL DISPLAY PANEL – 100 mg
ALWAYS DISPENSE WITH MEDICATION GUIDE
NDC 58151-576-93
Zoloft
30 Tablets Rx only
Store at 20°C to 25°C (68°F to
DOSAGE AND USESee accompanying
prescribing information.
prescribing information.
*Each tablet contains 111.9 mg
Distributed by:
© 2023 Viatris Inc.
Made in Germany
RUPJ576H
14PRINCIPAL DISPLAY PANEL – 20 mg/mL
ALWAYS DISPENSE WITH MEDICATION GUIDE
NDC 58151-601-35
Zoloft
Must Be Diluted
CALIBRATED DROPPER ENCLOSED
60 mL Rx only
Store at 20°C to 25°C (68°F to
STORE UPRIGHT.
DOSAGE AND USE
See accompanying
prescribing information.
See accompanying
prescribing information.
*Each mL of solution contains
Contains 12% alcohol.
THE PACKAGING OF THIS
Zoloft Oral Solution Must Be Diluted Before Use.
MIXING INSTRUCTIONS
Just before taking, use the dropper provided to remove the required amount of
ZOLOFT Oral Solution and mix with 4 oz (1/2 cup) of water, ginger ale, lemon/lime
soda, lemonade or orange juice ONLY. Do not mix ZOLOFT Oral Solution with
anything other than the liquids listed. At times, a slight haze may appear after
mixing; this is normal. The medicine should be given immediately after mixing.
Just before taking, use the dropper provided to remove the required amount of
ZOLOFT Oral Solution and mix with 4 oz (1/2 cup) of water, ginger ale, lemon/lime
soda, lemonade or orange juice ONLY. Do not mix ZOLOFT Oral Solution with
anything other than the liquids listed. At times, a slight haze may appear after
mixing; this is normal. The medicine should be given immediately after mixing.
DO NOT MIX IN ADVANCE.
Distributed by:
© 2023 Viatris Inc.
Made in Spain
ZOLOFT is a registered trademark of Viatris Specialty LLC, a Viatris Company.
