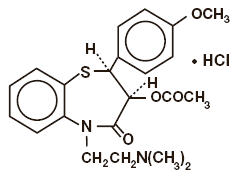
Diltiazem
What is Cardizem (Diltiazem)?
Approved To Treat
Top Global Experts



Related Clinical Trials
Summary: This phase I/II trial compares the effect of drugs that causes widening of blood vessels as a result of smooth muscle relaxation (vasodilator therapy) with isosorbide mononitrate, diltiazem or placebo to reduce vasotoxicity in patients with gastrointestinal cancer receiving fluoropyrimidine therapy. Some patients develop chest pain (possibly even a heart attack, a drop in heart function, or a rhyt...
Summary: Supraventricular tachycardia (SVT) is a dysrhythmia characterized rapid heart rate, typically with rapid onset. SVT accounts for over 50,000 emergency department visits per year. Of patients with regular, narrow-complex SVT, the mainstay of therapy includes adenosine and diltiazem. Adenosine is recommend by American and European guidelines as first-line therapy, however adenosine carries unique si...
Summary: This is a small, pilot study with a primary goal of assessing patient perceptions of two medication treatments for supraventricular tachycardia in adult patients treated in the Emergency Department.
Related Latest Advances
Brand Information
Bausch Health US, LLC
Bridgewater, NJ 08807 USA
Bausch Health Companies Inc.
Steinbach, MB R5G 1Z7, Canada