Optic Neuritis Treatments
Find Optic Neuritis Treatments
Enspryng
What is Enspryng (Satralizumab)?
Approved To Treat

Related Clinical Trials
Summary: CLUE is a prospective study to assess structural and functional changes of the brain, spinal cord, and optic nerve, as well as the inflammatory environment in patients with neuroinflammatory and demyelinating diseases. Participants will receive magnetic resonance (MR) techniques including DIR, DKI, QSM, Rs-fMRI, conventional sequences (T1WI/T2WI/FLAIR), and the MR metabolic SPICE sequence, and wil...
Summary: This study will primarily evaluate the pharmacokinetics of satralizumab in pediatric patients aged 2-11 years with anti-aquaporin-4 (AQP4) antibody seropositive neuromyelitis optica spectrum disorder (NMOSD). Efficacy, safety, tolerability, and pharmacodynamics will be evaluated in a descriptive manner, given the small number of patients who will be enrolled in this study.
Summary: The purpose of this study is to assess the efficacy, safety, PK, and PD of satralizumab in participants with NMDAR and LGI1 encephalitis.
Related Latest Advances
Brand Information
- A known hypersensitivity to satralizumab or any of the inactive ingredients
- Active Hepatitis B infection
- Active or untreated latent tuberculosis
- Infections
- Elevated Liver Enzymes
- Decreased Neutrophil Counts
- Hypersensitivity Reactions
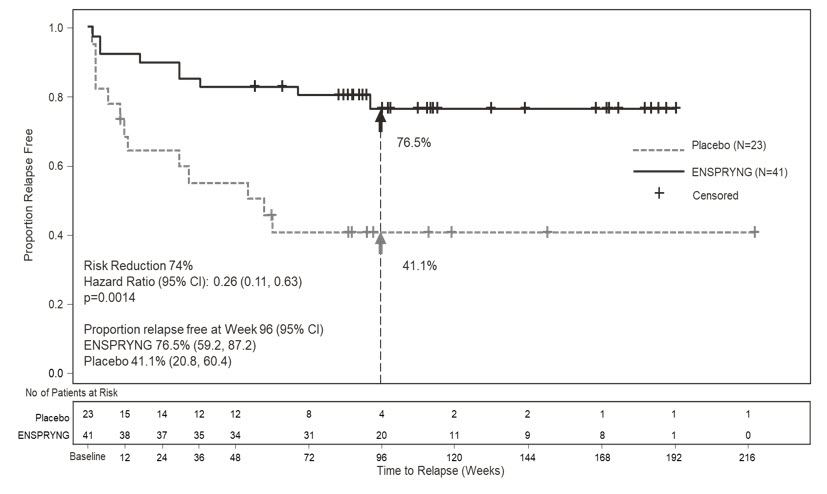
- Study 1: Clinical evidence of 1 relapse in the previous 12 months
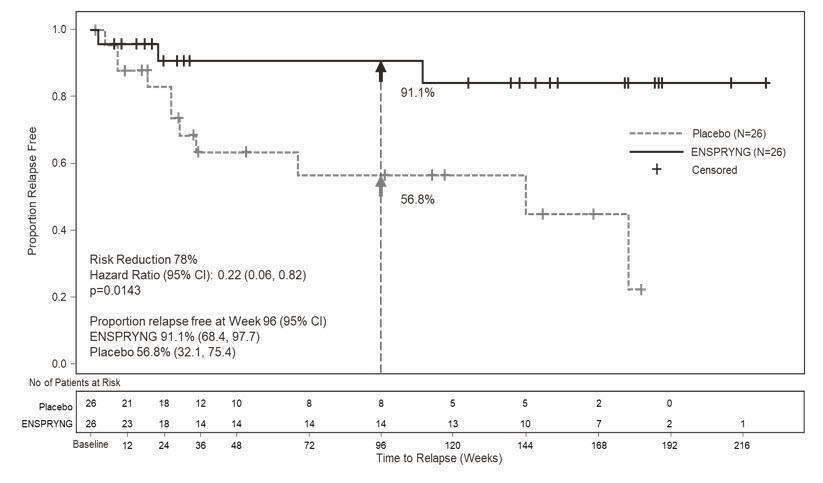
- Study 2: Clinical evidence of at least 2 relapses in the previous 2 years, at least one of which must have occurred in the previous year
- EDSS score of 0 to 6.5 (both studies)
- Study 1: Patients were excluded if previously treated with IST within an interval specified for each such therapy
- Study 2: One of the following baseline treatments at a stable dose as a monotherapy for 8 weeks prior to baseline: azathioprine, mycophenolate mofetil, oral corticosteroids
(satralizumab-mwge)
Injection, for subcutaneous use
single-dose prefilled syringe
- Do not use ENSPRYNG prefilled syringe until your healthcare provider has trained you or your caregiver on the right way to inject.
- Do not share your ENSPRYNG syringe with other people. You may give them a serious infection or get a serious infection from them.
- Do not use if the expiration (EXP) date has passed.
- Do not use if the seal on the carton have been broken.
- Do not try to take the syringe apart at any time.
- Do not take the needle cap off until you are ready to inject ENSPRYNG.
- Do not use the syringe if it has been dropped or damaged.
- Do not re-use the same syringe. Each prefilled syringe can be used only 1 time.
- Do not inject through clothing.
- Store ENSPRYNG prefilled syringe in the refrigerator between
- The ENSPRYNG carton can be stored at room temperature up to 86°F (30°C) for up to 8 days. If ENSPRYNG is removed from and returned to the refrigerator, the total combined time out of refrigeration should not be more than 8 days.
- Keep the syringe in its original carton away from direct sunlight.
- Always keep the syringe dry.
- Do not freeze ENSPRYNG. Do not use the prefilled syringe if it has been frozen.
- Do not shake.
- Throw away (dispose of) the prefilled syringe if it has been frozen, exposed to light or temperatures above 86°F (30°C), or has been out of the refrigerator for more than 8 days.
- Keep the ENSPRYNG syringe and all medicines out of the reach of children.
- 1 prefilled syringe for 1-time use only.
- 1 alcohol pad
- 1 sterile cotton ball or gauze
- 1 small bandage
- 1 FDA-cleared, puncture-resistant sharps container for safe disposal of the needle cap and used syringe. See
- Take the carton containing the syringe out of the refrigerator and place it on a clean, flat work surface (like a table).
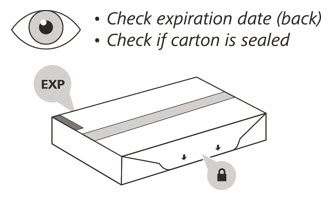
- Check the expiration (EXP) date on the back of the carton
- Check the front of the carton to make sure it is sealed
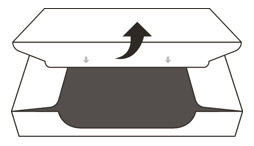
- Open the sealed carton
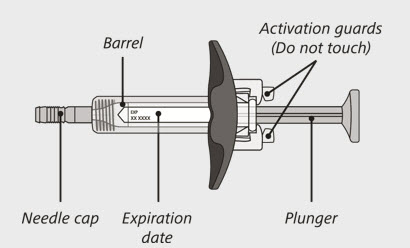
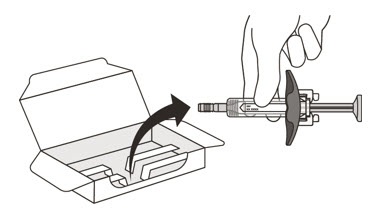
- Carefully lift the syringe out of the carton by holding the barrel
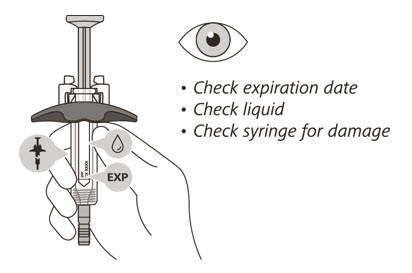
- Check the expiration date on the syringe.
- Check the syringe for any damage.
- Check that the liquid through the viewing window is clear and colorless to slightly yellow.
- After you have checked the syringe, place it on a clean, flat work surface (like a table) for

- Wash your hands with soap and water.

- Choose your injection site in either:
- Wipe the injection site with an alcohol pad and let it air dry.

- Hold the barrel of the syringe between your thumb and index finger. With your other hand, pull the needle cap straight off. You may see a drop of liquid at the end of the needle. This is normal and will not affect your dose
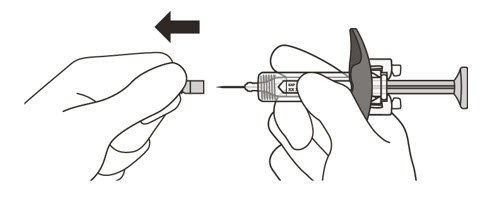
- Throw away the needle cap in a puncture-resistant sharps container immediately. See
- Hold the barrel of the syringe using your thumb and index finger. With your other hand, pinch the area of skin you have cleaned
- Use a quick, dart-like motion to insert the needle at an angle between 45° to 90°
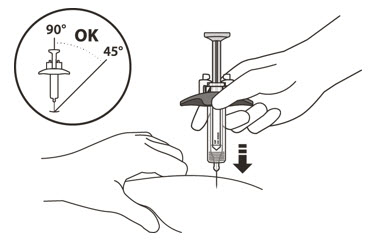
- After the needle is inserted, let go of the pinched skin.
- Slowly inject all of the medicine by gently pushing the plunger all the way down until it touches the activation guards
- Gently release the plunger and allow the needle to come out of the skin at the same angle it was inserted
- There may be a little bleeding at the injection site. You can press a cotton ball or gauze over the injection site but
- Put your used syringe in an FDA-cleared sharps disposal container immediately after use
(satralizumab-mwge)
injection, for subcutaneous use
single-dose prefilled autoinjector
- Do not use ENSPRYNG autoinjector until your healthcare provider has trained you or your caregiver on the right way to inject.
- Do not use if the expiration (EXP) date has passed.
- Do not use if the seals on the carton have been broken.
- Do not try to take the autoinjector apart at any time.
- Do not remove the cap until you are ready to inject.
- Do not use if the autoinjector has been damaged or dropped.
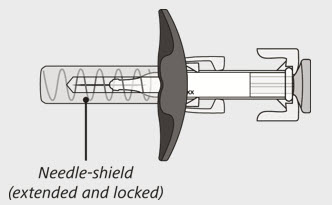
- Do not touch or clean the green needle shield.
- Do not try to re-use the same autoinjector. Each prefilled autoinjector can be used only one time.
- Do not inject through clothing.
- Store ENSPRYNG autoinjector in the original carton in the refrigerator between 36°F to 46°F (2°C to 8°C) until ready to use.
- The ENSPRYNG carton can be stored at room temperature up to 86°F (30°C) for up to 8 days. If ENSPRYNG is removed from and returned to the refrigerator, the total combined time out of the refrigerator should not be more than 8 days.
- Keep the autoinjector in the original carton away from direct sunlight.
- Do not freeze ENSPRYNG. Do not use the autoinjector if it has been frozen.
- Do not shake.
- Throw away (dispose of) the autoinjector if it has been frozen, exposed to light or temperatures above 86°F (30°C), or has been out of the refrigerator for more than 8 days.
- Keep ENSPRYNG and all medicines out of the reach of children.

- Gather supplies needed for your injection.
- ENSPRYNG autoinjector
- 1 alcohol pad
- 1 sterile cotton ball or gauze
- 1 small adhesive bandage
- 1 sharps disposal container (See
- Take the ENSPRYNG autoinjector carton out of the refrigerator.
- Open the carton and take the autoinjector out of the tray.
- Check the expiration (EXP) date on the autoinjector.
- Do not inject if the expiration date (EXP) has passed.
- Check the medicine through the viewing window. The medicine should be clear or slightly yellow. There should be no particles in it.
- Do not inject if the medicine looks cloudy, discolored, or has particles in it. You may see small air bubbles. This is normal and you should not try to remove them.
- Check the autoinjector for any damage.
- Do not use if the autoinjector is cracked or broken.
- Place the autoinjector on a clean, flat surface (like a table) for 30 minutes. This allows the medicine to reach room temperature.
- Do not speed up the warming process in any way, such as using a microwave, warm water, or direct sunlight.
- Do not remove the cap until you are ready to inject.
- You can inject ENSPRYNG in the stomach area (abdomen) or front of the thigh.
- Do not inject into the 2 inches (5 cm) area around the belly button.
- Do not inject into moles, scars, or areas where the skin is tender, bruised, red, hard, or not intact.
- Wash your hands with soap and water.
- Clean the injection site with an alcohol pad and let it air dry.
- Do not fan or blow on the area you have cleaned.
- Do not touch the injection site again before you inject.
- Hold the autoinjector with the cap pointing up. Then pull the cap straight off.
- Do not clean the green needle shield. This may activate the autoinjector.
- Do not put the cap back on after it has been removed. This may activate the autoinjector.

- Hold the autoinjector so that you can
- Do not change the angle of the injection.
- Push firmly and hold down the autoinjector against the skin.
The first click indicates the injection has started.
- The
- Do not lift the autoinjector if the green plunger is moving. This may cause a loss of medicine.
- Keep holding down the autoinjector firmly.
- Watch the green plunger as it moves down. Or check if the green plunger has already filled the entire viewing window (See Step 15).
- Before removing the autoinjector from the injection site, check that the green plunger fills the viewing window entirely.
- If the green plunger does not fill the viewing window, you may not have received the full dose. Safely throw away (dispose of) the autoinjector in a sharps disposal container (See Step 17) and contact your healthcare provider.
- Remove the autoinjector by lifting it straight up from the skin.
- The green needle shield will lock into place, covering the needle when the injection is complete.
- Put the used autoinjector and the cap in an FDA-cleared sharps disposal container right away after use.
- Do not throw away (dispose of) the autoinjector in your household trash.
- There may be a small amount of blood or medicine at the injection site.
- Do not rub or massage the area where you have injected.

