Paroxysmal Supraventricular Tachycardia (PSVT) Treatments
Find Paroxysmal Supraventricular Tachycardia (PSVT) Treatments
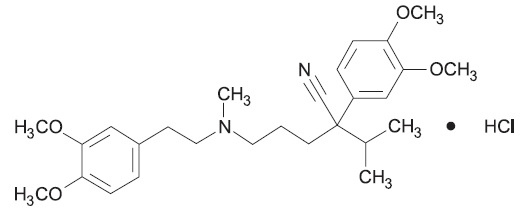
Verapamil
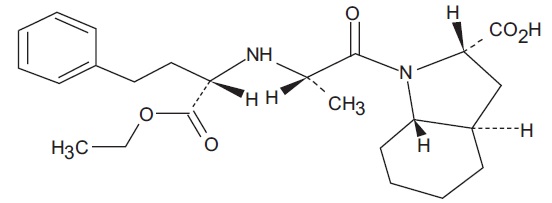
What is Trandolapril (Verapamil)?
Approved To Treat





Related Clinical Trials
Summary: This multi-center randomized controlled trial will assess the safety and efficacy of ATG followed by either adalimumab or verapamil in preserving insulin secretion 2 years from randomization in persons aged 9 to \<21 with recent-onset stage 3 T1D.
Summary: Over half of women in the US who are breastfeeding their infants take prescription drugs. You are being asked to participate in this study because you are breastfeeding your infant and are currently taking, as part of your medical care, at least one of the drugs we are studying. We are interested in studying drugs commonly prescribed to women who are breastfeeding so we can learn more about the am...
Summary: Heart failure (HF) is a chronic condition that is characterized by a weakened and enlarged heart. It typically causes symptoms such as breathlessness and swelling of the legs, and it is a serious illness that shortens life expectancy. In recent years, new medicines have been developed that can improve heart function and help patients with HF live longer. HF patients with reduced heart function typ...
Related Latest Advances
Brand Information
- When pregnancy is detected, discontinue trandolapril and verapamil hydrochloride extended-release tablets as soon as possible.
- Drugs that act directly on the renin-angiotensin system can cause injury and death to the developing fetus (see WARNINGS: .
- Severe left ventricular dysfunction (see
- Hypotension (systolic pressure less than 90 mmHg) or cardiogenic shock.
- Sick sinus syndrome (except in patients with a functioning artificial ventricular pacemaker).
- Second- or third-degree AV block (except in patients with a functioning artificial ventricular pacemaker).
- Patients with atrial flutter or atrial fibrillation and an accessory bypass tract (e.g. Wolff-Parkinson-White, Lown-Ganong-Levine syndromes) (see
- Patients taking flibanserin (see
NDC 68462-294-01 — bottles of 100
NDC 68462-294-10 — bottles of 1000
NDC 68462-295-01 — bottles of 100
NDC 68462-295-10 — bottles of 1000
NDC 68462-296-01 — bottles of 100
NDC 68462-296-10 — bottles of 1000
NDC 68462-329-10 — bottles of 1000



